

Cardiovascular profiling in the diabetic continuum: results from the population-based Gutenberg Health Study
- PMID: 34169342
- PMCID: PMC8873120
- DOI: 10.1007/s00392-021-01879-y
Cardiovascular profiling in the diabetic continuum: results from the population-based Gutenberg Health Study
Abstract
Aims: To assess the prevalence of type 2 diabetes mellitus (T2DM) and prediabetes in the general population and to investigate the associated cardiovascular burden and clinical outcome.
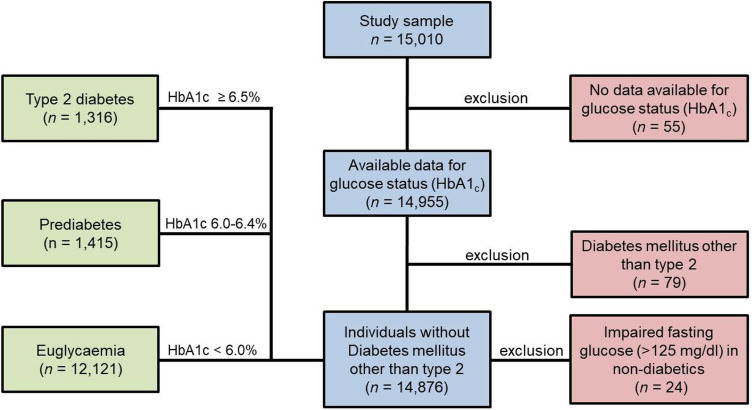
Methods and results: The study sample comprised 15,010 individuals aged 35-74 years of the population-based Gutenberg Health Study. Subjects were classified into euglycaemia, prediabetes and T2DM according to clinical and metabolic (HbA1c) information. The prevalence of prediabetes was 9.5% (n = 1415) and of T2DM 8.9% (n = 1316). Prediabetes and T2DM showed a significantly increased prevalence ratio (PR) for age, obesity, active smoking, dyslipidemia, and arterial hypertension compared to euglycaemia (for all, P < 0.0001). In a robust Poisson regression analysis, prediabetes was established as an independent predictor of clinically-prevalent cardiovascular disease (PRprediabetes 1.20, 95% CI 1.07-1.35, P = 0.002) and represented as a risk factor for asymptomatic cardiovascular organ damage independent of traditional risk factors (PR 1.04, 95% CI 1.01-1.08, P = 0.025). Prediabetes was associated with a 1.5-fold increased 10-year risk for cardiovascular disease compared to euglycaemia. In Cox regression analysis, prediabetes (HR 2.10, 95% CI 1.76-2.51, P < 0.0001) and T2DM (HR 4.28, 95% CI 3.73-4.92, P < 0.0001) indicated for an increased risk of death. After adjustment for age, sex and traditional cardiovascular risk factors, only T2DM (HR 1.89, 95% CI 1.63-2.20, P < 0.0001) remained independently associated with increased all-cause mortality.
Conclusion: Besides T2DM, also prediabetes inherits a significant cardiovascular burden, which translates into poor clinical outcome and indicates the need for new concepts regarding the prevention of cardiometabolic disorders.
Keywords: All-cause mortality; Asymptomatic organ damage; Cardiovascular disease; Disease prevention; Prediabetes; Type 2 diabetes mellitus.
© 2021. The Author(s).
Conflict of interest statement
J.H.P. received funding for lecturing by Bayer AG and Boehringer Ingelheim outside the topic of this work. P.S.W. reports the submitted work grants from Bayer AG, non-financial grants from Philips Medical Systems, grants and consulting fees from Boehringer Ingelheim, grants and consulting fees from Novartis Pharma, grants and consulting fees from Sanofi-Aventis, grants, consulting and lecturing fees from Bayer Health Care, grants from Daiichi Sankyo Europe, consulting fees from Astra Zeneca, consulting fees and non-financial support from Diasorin and non-financial support from I.E.M., outside the submitted work. S.O.T has received lecture fees for Philips AG outside the submitted work. All other authors declare no disclosures that could be perceived as conflict of interest in the context of the present work.
Figures




References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
