

Tailored Versus Standard Hydration to Prevent Acute Kidney Injury After Percutaneous Coronary Intervention: Network Meta-Analysis
- PMID: 34169747
- PMCID: PMC8403299
- DOI: 10.1161/JAHA.121.021342
Tailored Versus Standard Hydration to Prevent Acute Kidney Injury After Percutaneous Coronary Intervention: Network Meta-Analysis
Abstract
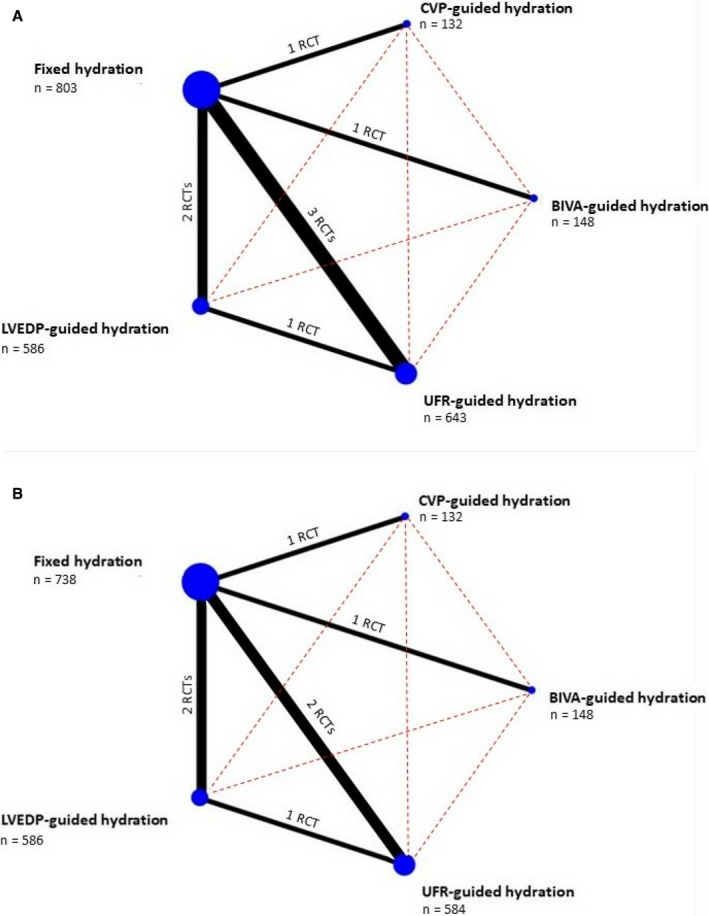
Background Contrast-induced acute kidney injury (CI-AKI) is a serious complication after percutaneous coronary intervention. The mainstay of CI-AKI prevention is represented by intravenous hydration. Tailoring infusion rate to patient volume status has emerged as advantageous over fixed infusion-rate hydration strategies. Methods and Results A systematic review and network meta-analysis with a frequentist approach were conducted. A total of 8 randomized controlled trials comprising 2312 patients comparing fixed versus tailored hydration strategies to prevent CI-AKI after percutaneous coronary intervention were included in the final analysis. Tailored hydration strategies included urine flow rate-guided, central venous pressure-guided, left ventricular end-diastolic pressure-guided, and bioimpedance vector analysis-guided hydration. Primary endpoint was CI-AKI incidence. Safety endpoint was incidence of pulmonary edema. Urine flow rate-guided and central venous pressure-guided hydration were associated with a lower incidence of CI-AKI compared with fixed-rate hydration (odds ratio [OR], 0.32 [95% CI, 0.19-0.54] and OR, 0.45 [95% CI, 0.21-0.97]). No significant difference in pulmonary edema incidence was observed between the different hydration strategies. P score analysis showed that urine flow rate-guided hydration is advantageous in terms of both CI-AKI prevention and pulmonary edema incidence when compared with other approaches. Conclusions Currently available hydration strategies tailored on patients' volume status appear to offer an advantage over guideline-supported fixed-rate hydration for CI-AKI prevention after percutaneous coronary intervention. Current evidence suggests that urine flow rate-guided hydration as the most convenient strategy in terms of effectiveness and safety.
Keywords: contrast‐induced acute kidney injury; coronary angiography; hydration; percutaneous coronary intervention.
Conflict of interest statement
Dr Brilakis reports consulting/speaker honoraria from Abbott Vascular, American Heart Association (
Figures




References
-
- Tsai TT, Patel UD, Chang TI, Kennedy KF, Masoudi FA, Matheny ME, Kosiborod M, Amin AP, Messenger JC, Rumsfeld JS, et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the NCDR Cath‐PCI registry. JACC Cardiovasc Interv. 2014;7:1–9. - PMC - PubMed
-
- Valle JA, McCoy LA, Maddox TM, Rumsfeld JS, Ho PM, Casserly IP, Nallamothu BK, Roe MT, Tsai TT, Messenger JC. Longitudinal risk of adverse events in patients with acute kidney injury after percutaneous coronary intervention: insights from the National Cardiovascular Data Registry. Circ Cardiovasc Interv. 2017;10:e004439. DOI: 10.1161/CIRCINTERVENTIONS.116.004439. - DOI - PubMed
-
- Almendarez M, Gurm HS, Mariani J, Montorfano M, Brilakis ES, Mehran R, Azzalini L. Procedural strategies to reduce the incidence of contrast‐induced acute kidney injury during percutaneous coronary intervention. JACC Cardiovasc Interv. 2019;12:1877–1888. DOI: 10.1016/j.jcin.2019.04.055. - DOI - PubMed
-
- Wohlin C, ACM (Association for Computing Machinery) . Guidelines for snowballing in systematic literature studies and a replication in software engineering. Proceedings of the 18th International Conference on Evaluation and Assessment in Software Engineering. New York, NY: Association for Computing Machinery; 2014: 1–10. DOI: 10.1145/2601248.2601268. - DOI
-
- Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, Ioannidis JPA, Straus S, Thorlund K, Jansen JP, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta‐analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162:777–784. DOI: 10.7326/M14-2385. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
