

Pharmacodynamics of cerebrospinal fluid asparagine after asparaginase
- PMID: 34170389
- PMCID: PMC8424750
- DOI: 10.1007/s00280-021-04315-0
Pharmacodynamics of cerebrospinal fluid asparagine after asparaginase
Abstract
Purpose: We evaluated effects of asparaginase dosage, schedule, and formulation on CSF asparagine in children with acute lymphoblastic leukemia (ALL).
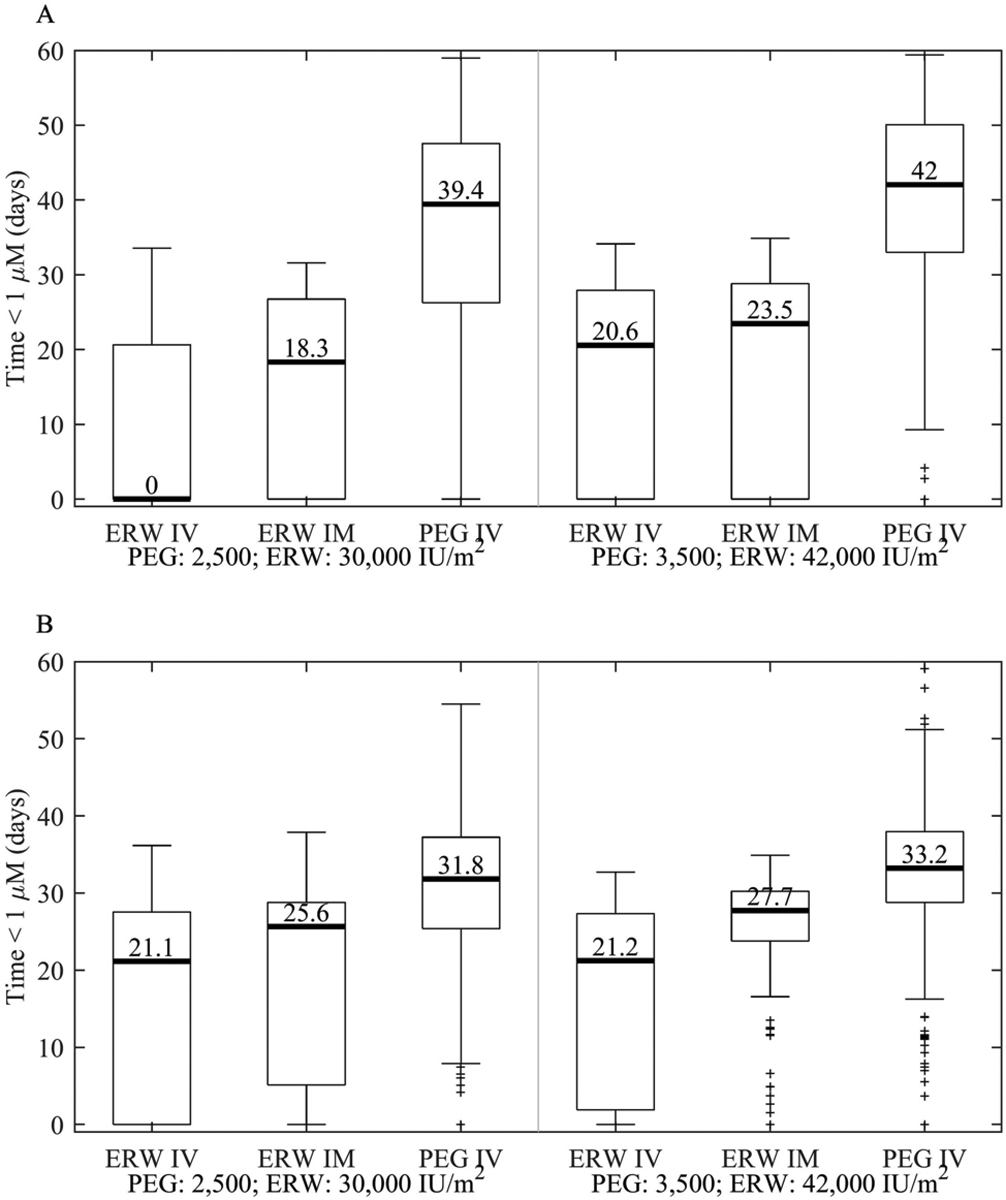
Methods: We evaluated CSF asparagine (2114 samples) and serum asparaginase (5007 samples) in 482 children with ALL treated on the Total XVI study (NCT00549848). Patients received one or two 3000 IU/m2 IV pegaspargase doses during induction and were then randomized in continuation to receive 2500 IU/m2 or 3500 IU/m2 IV intermittently (four doses) on the low-risk (LR) or continuously (15 doses) on the standard/high risk (SHR) arms. A pharmacokinetic-pharmacodynamic model was used to estimate the duration of CSF asparagine depletion below 1 uM.
Results: During induction, CSF asparagine depletion after two doses of pegaspargase was twice as long as one dose (median 30.7 vs 15.3 days, p < 0.001). During continuation, the higher dose increased the CSF asparagine depletion duration by only 9% on the LR and 1% in the SHR arm, consistent with the nonlinear pharmacokinetics of serum asparaginase. Pegaspargase caused a longer CSF asparagine depletion duration (1.3-5.3-fold) compared to those who were switched to erwinase (p < 0.001). The median (quartile range) serum asparaginase activity needed to maintain CSF asparagine below 1 µM was 0.44 (0.20, 0.99) IU/mL. Although rare, CNS relapse was higher with decreased CSF asparagine depletion (p = 0.0486); there was no association with relapse at any site (p = 0.3).
Conclusions: The number of pegaspargase doses has a stronger influence on CSF asparagine depletion than did dosage, pegaspargase depleted CSF asparagine longer than erwinase, and CSF asparagine depletion may prevent CNS relapses.
Keywords: Acute lymphoblastic leukemia; Asparagine; Cerebrospinal fluid; Erwinia asparaginase; Pediatric; Pegylated asparaginase; Pharmacodynamics; Pharmacokinetics.
© 2021. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Figures



Comment in
-
Comment on "Pharmacodynamics of cerebrospinal fluid asparagine after asparaginase".Cancer Chemother Pharmacol. 2021 Nov;88(5):919-920. doi: 10.1007/s00280-021-04345-8. Epub 2021 Sep 1. Cancer Chemother Pharmacol. 2021. PMID: 34468793 No abstract available.
References
-
- Jarrar M, Gaynon PS, Periclou AP, Fu C, Harris RE, Stram D, Altman A, Bostrom B, Breneman J, Steele D, Trigg M, Zipf T, Avramis VI (2006) Asparagine depletion after pegylated E. coli asparaginase treatment and induction outcome in children with acute lymphoblastic leukemia in first bone marrow relapse: a Children’s Oncology Group study (CCG-1941). Pediatr Blood Cancer 47 (2):141–146. doi:10.1002/pbc.20713 - DOI - PubMed
-
- Avramis VI, Sencer S, Periclou AP, Sather H, Bostrom BC, Cohen LJ, Ettinger AG, Ettinger LJ, Franklin J, Gaynon PS, Hilden JM, Lange B, Majlessipour F, Mathew P, Needle M, Neglia J, Reaman G, Holcenberg JS, Stork L (2002) A randomized comparison of native Escherichia coli asparaginase and polyethylene glycol conjugated asparaginase for treatment of children with newly diagnosed standard-risk acute lymphoblastic leukemia: a Children’s Cancer Group study. Blood 99 (6):1986–1994. doi:10.1182/blood.v99.6.1986 - DOI - PubMed
-
- Abshire TC, Pollock BH, Billett AL, Bradley P, Buchanan GR (2000) Weekly polyethylene glycol conjugated L-asparaginase compared with biweekly dosing produces superior induction remission rates in childhood relapsed acute lymphoblastic leukemia: a Pediatric Oncology Group Study. Blood 96 (5):1709–1715 - PubMed
-
- Silverman LB, Gelber RD, Dalton VK, Asselin BL, Barr RD, Clavell LA, Hurwitz CA, Moghrabi A, Samson Y, Schorin MA, Arkin S, Declerck L, Cohen HJ, Sallan SE (2001) Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91–01. Blood 97 (5):1211–1218. doi:10.1182/blood.v97.5.1211 - DOI - PubMed
-
- Pession A, Valsecchi MG, Masera G, Kamps WA, Magyarosy E, Rizzari C, van Wering ER, Lo Nigro L, van der Does A, Locatelli F, Basso G, Arico M (2005) Long-term results of a randomized trial on extended use of high dose L-asparaginase for standard risk childhood acute lymphoblastic leukemia. J Clin Oncol 23 (28):7161–7167. doi:10.1200/JCO.2005.11.411 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
