

OUTpatient intravenous LASix Trial in reducing hospitalization for acute decompensated heart failure (OUTLAST)
- PMID: 34170908
- PMCID: PMC8232441
- DOI: 10.1371/journal.pone.0253014
OUTpatient intravenous LASix Trial in reducing hospitalization for acute decompensated heart failure (OUTLAST)
Abstract
Background: Hospitalization for acute decompensated heart failure (ADHF) remains a major source of morbidity and mortality. The current study aimed to investigate the feasibility, safety, and efficacy of outpatient furosemide intravenous (IV) infusion following hospitalization for ADHF.
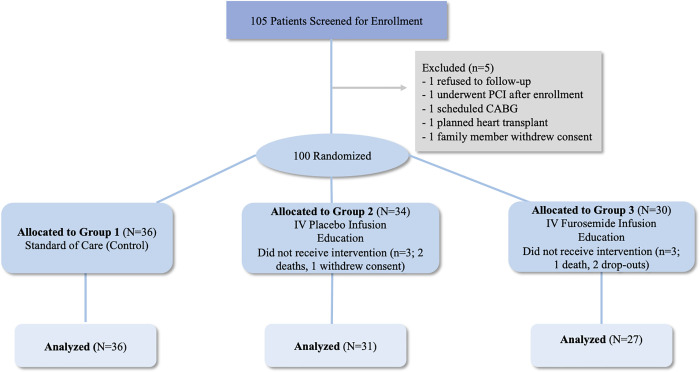
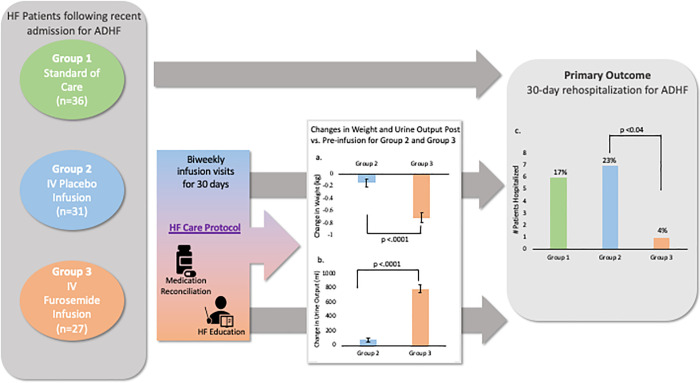
Methods: In a single center, prospective, randomized, double-blind study, 100 patients were randomized to receive standard of care (Group 1), IV placebo infusion (Group 2), or IV furosemide infusion (Group 3) over 3h, biweekly for a one-month period following ADHF hospitalization. Patients in Groups 2/3 also received a comprehensive HF-care protocol including bi-weekly clinic visits for dose-adjusted IV-diuretics, medication adjustment and education. Echocardiography, quality of life and depression questionnaires were performed at baseline and 30-day follow-up. The primary outcome was 30-day re-hospitalization for ADHF.
Results: Overall, a total of 94 patients were included in the study (mean age 64 years, 56% males, 69% African American). There were a total of 14 (15%) hospitalizations for ADHF at 30 days, 6 (17.1%) in Group 1, 7 (22.6%) in Group 2, and 1 (3.7%) in Group 3 (overall p = 0.11; p = 0.037 comparing Groups 2 and 3). Patients receiving IV furosemide infusion experienced significantly greater urine output and weight loss compared to those receiving placebo without any significant increase creatinine and no significant between group differences in echocardiography parameters, KCCQ or depression scores.
Conclusion: The use of a standardized protocol of outpatient IV furosemide infusion for a one-month period following hospitalization for ADHF was found to be safe and efficacious in reducing 30-day re-hospitalization.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
