

Skin infections due to Panton-Valentine leukocidin (PVL)-producing S. aureus-Cost effectiveness of outpatient treatment
- PMID: 34170945
- PMCID: PMC8232536
- DOI: 10.1371/journal.pone.0253633
Skin infections due to Panton-Valentine leukocidin (PVL)-producing S. aureus-Cost effectiveness of outpatient treatment
Abstract
Introduction: Skin and soft tissue infections (SSTI) caused by Panton-Valentine leukocidin (PVL)-producing strains of Staphylococcus aureus (PVL-SA) are associated with recurrent skin abscesses. Secondary prevention, in conjunction with primary treatment of the infection, focuses on topical decolonization. Topical decolonization is a standard procedure in cases of recurrent PVL-SA skin infections and is recommended in international guidelines. However, this outpatient treatment is often not fully reimbursed by health insurance providers, which may interfere with successful PVL-SA decolonization.
Aim: Our goal was to estimate the cost effectiveness of outpatient decolonization of patients with recurrent PVL-SA skin infections. We calculated the average cost of treatment for PVL-SA per outpatient decolonization procedure as well as per in-hospital stay.
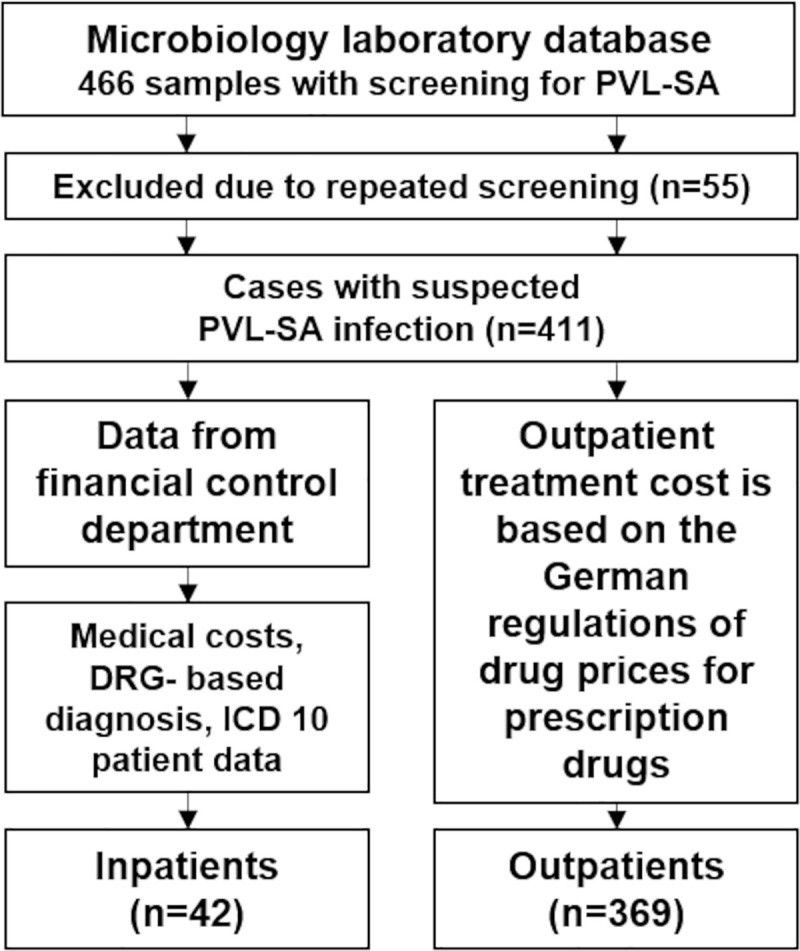
Methods: The study was conducted between 2014 and 2018 at a German tertiary care university hospital. The cohort analyzed was obtained from the hospital's microbiology laboratory database. Data on medical costs, DRG-based diagnoses, and ICD-10 patient data was obtained from the hospital's financial controlling department. We calculated the average cost of treatment for patients admitted for treatment of PVL-SA induced skin infections. The cost of outpatient treatment is based on the German regulations of drug prices for prescription drugs.
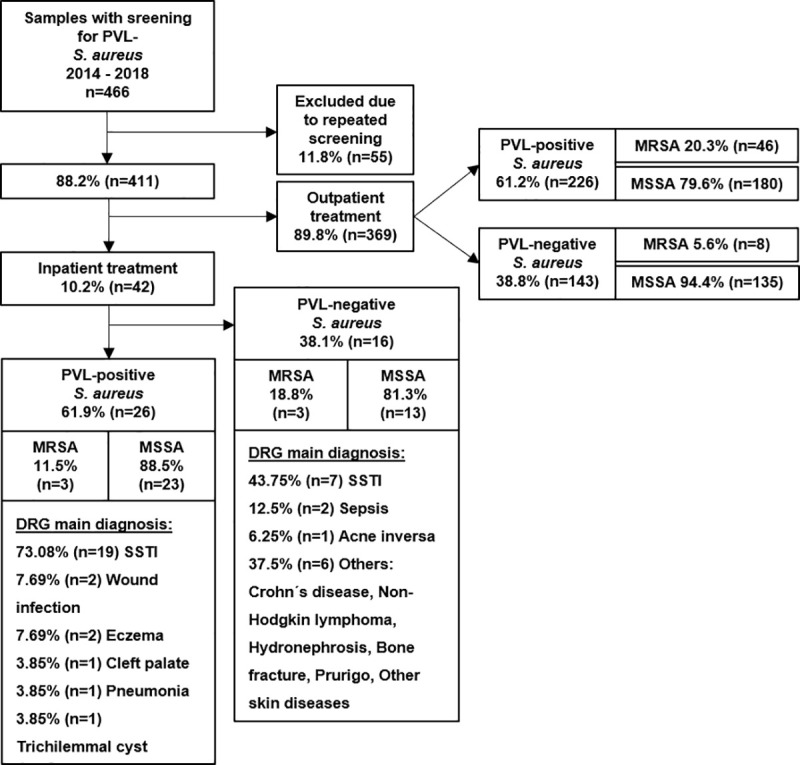
Results: We analyzed a total of n = 466 swabs from n = 411 patients with recurrent skin infections suspected of carrying PVL-SA. PVL-SA was detected in 61.3% of all patients included in the study. Of those isolates, 80.6% were methicillin-susceptible, 19.4% methicillin-resistant. 89.8% of all patients were treated as outpatients. In 73.0% of inpatients colonized with PVL-SA the main diagnosis was SSTI. The median length of stay was 5.5 days for inpatients colonized with PVL-SA whose main diagnosis SSTI; the average cost was €2,283. The estimated costs per decolonization procedure in outpatients ranged from €50-€110, depending on the products used.
Conclusion: Our data shows that outpatient decolonization offers a highly cost-effective secondary prevention strategy, which may prevent costly inpatient treatments. Therefore, health insurance companies should consider providing coverage of outpatient treatment of recurrent PVL-SA skin and soft tissue infections.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Wiese-Posselt M, Heuck D, Draeger A, Mielke M, Witte W, Ammon A, et al. Successful termination of a furunculosis outbreak due to lukS-lukF-positive, methicillin-susceptible Staphylococcus aureus in a German village by stringent decolonization, 2002–2005. Clin Infect Dis 2007; 44(11):e88–95. doi: 10.1086/517503 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
