

Depression and anxiety in recurrent giant cell tumor of bone
- PMID: 34171055
- PMCID: PMC8343577
- DOI: 10.47162/RJME.61.4.08
Depression and anxiety in recurrent giant cell tumor of bone
Abstract
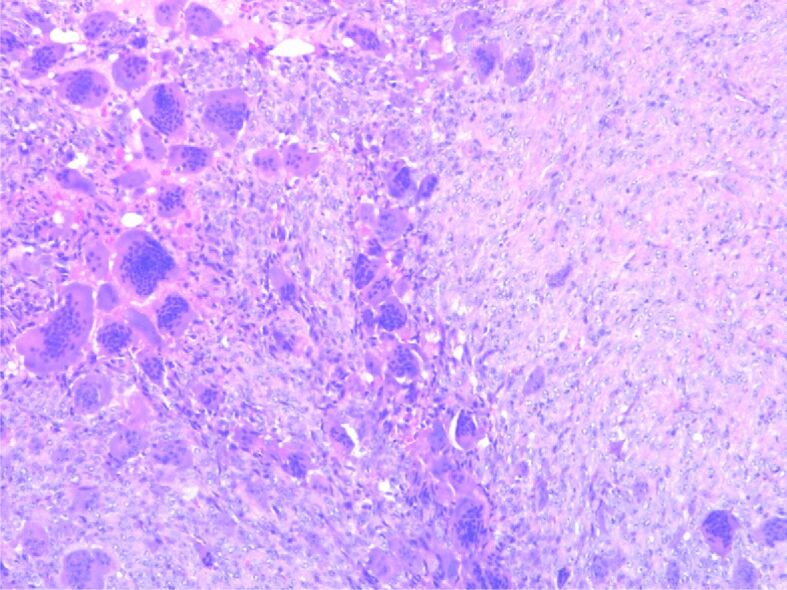
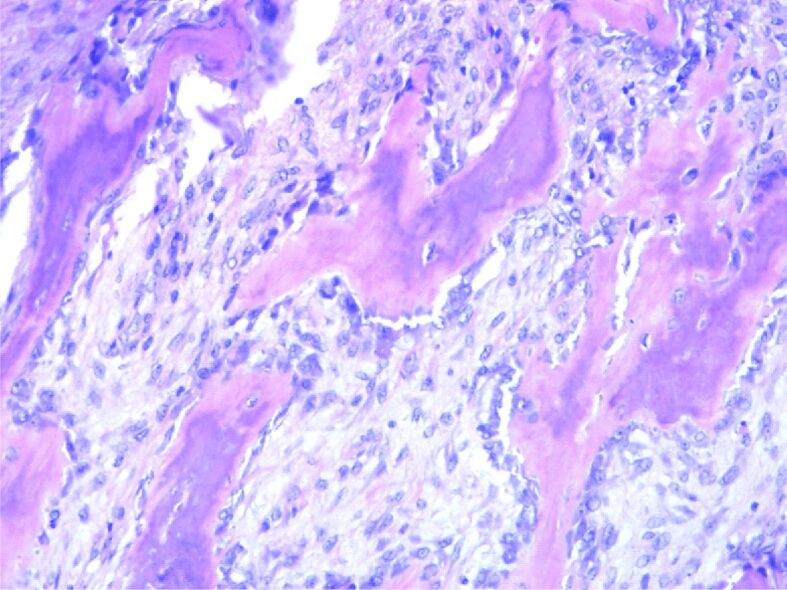
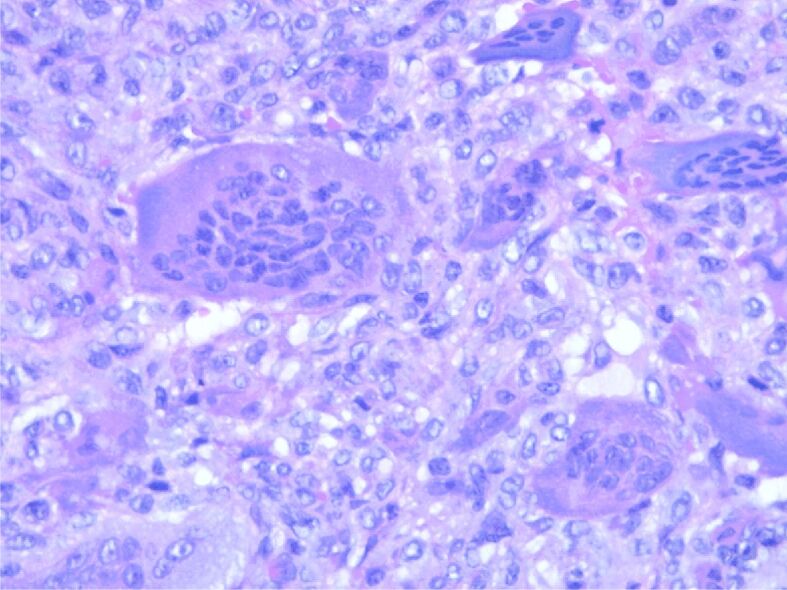
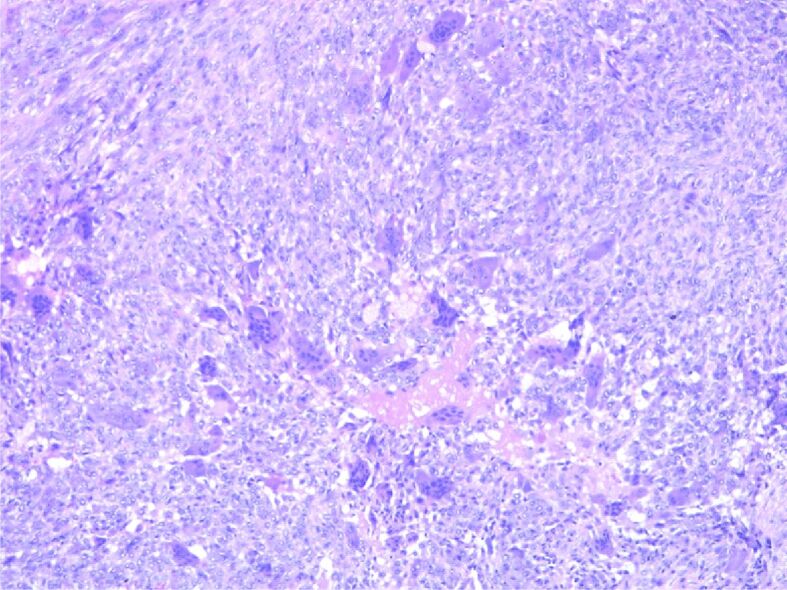
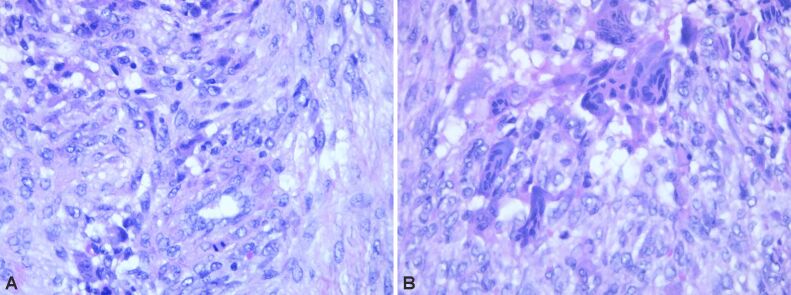
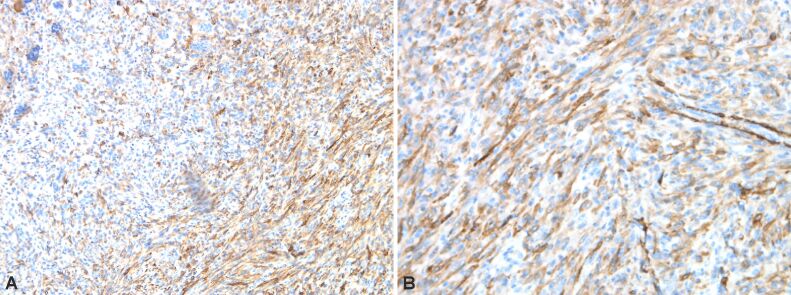
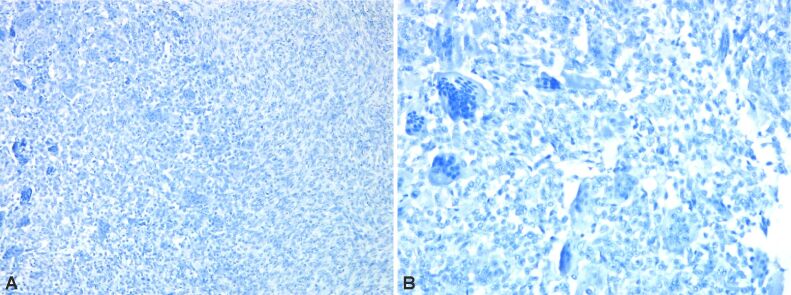
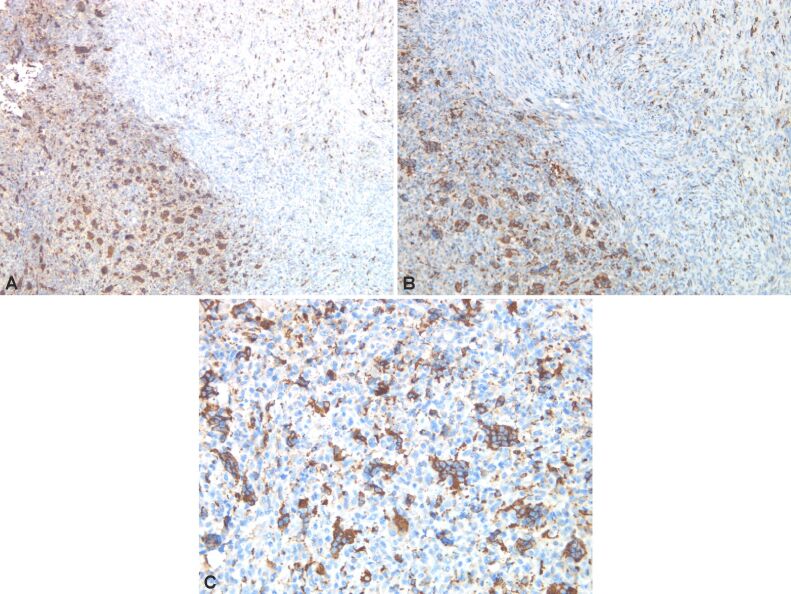
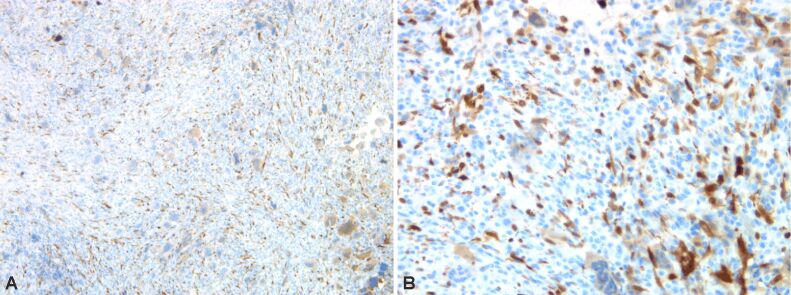
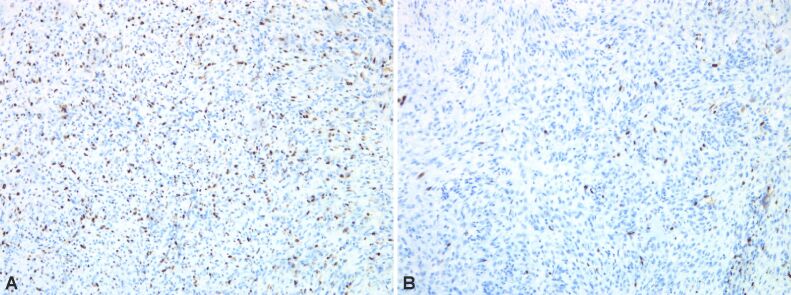
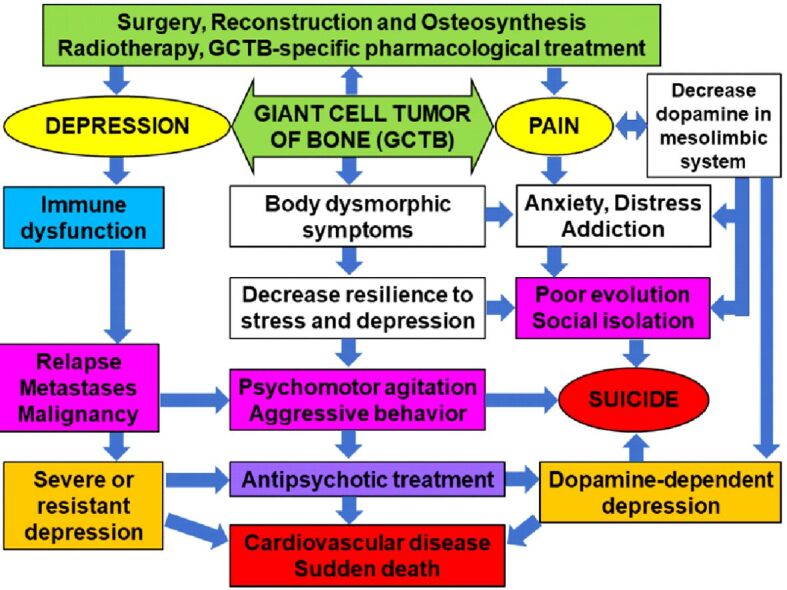
Giant cell tumor of bone (GCTB) is a benign neoplasia more frequently encountered in young females. The pathogenic and evolutionary dynamics of the disease is strongly influenced by the presence of depression and cellular mechanisms, especially proinflammatory and immune. Although it is not a malignant tumor, it is often recurrent, which determines a high level of depression, anxiety, and fear of the patients. Cytokine mechanisms, especially through increased tumor necrosis factor alpha (TNFα) and interleukin-6 (IL-6), as well as the involvement of the receptor activator of nuclear factor-kappa B (RANK)-RANK ligand (RANK-L) system, can be correlated with the risk of malignancy. Unfavorable evolution is associated with persistent pain, difficulties of movement and body dysmorphic symptoms. The diagnosis is based mainly on histopathological (HP) assessment. The patients can be treated with pharmacological agents (Denosumab), surgery with tumor excision, reconstruction or osteosynthesis, and radiotherapy. Patients with GCTB require HP and imaging evaluations, especially of relapses, to detect the risk of metastasis or malignancy, simultaneously with psychological and psychiatric monitoring to detect depression, addictive behaviors, and suicide risk. It is necessary to evaluate in a multidisciplinary team to avoid unfavorable oncological and psychiatric developments. Through its clinical, HP, and therapeutic features, GCTB has multiple connections with the psychological and psychopathological dimension.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures
Similar articles
-
Clinical outcome of recurrent giant cell tumor of the extremity in the era before molecular target therapy: the Japanese Musculoskeletal Oncology Group study.BMC Musculoskelet Disord. 2016 Jul 22;17:306. doi: 10.1186/s12891-016-1163-z. BMC Musculoskelet Disord. 2016. PMID: 27448567 Free PMC article.
-
Short-term Preoperative Denosumab With Surgery in Unresectable or Recurrent Giant Cell Tumor of Bone.Orthop Surg. 2019 Dec;11(6):1101-1108. doi: 10.1111/os.12561. Epub 2019 Nov 25. Orthop Surg. 2019. PMID: 31762217 Free PMC article.
-
Denosumab induces tumor reduction and bone formation in patients with giant-cell tumor of bone.Clin Cancer Res. 2012 Aug 15;18(16):4415-24. doi: 10.1158/1078-0432.CCR-12-0578. Epub 2012 Jun 18. Clin Cancer Res. 2012. PMID: 22711702 Clinical Trial.
-
Preoperative Denosumab plus Surgery in the Management of Giant Cell Tumor of Bone: A Comprehensive Narrative Literature Review.Gulf J Oncolog. 2019 May;1(30):67-75. Gulf J Oncolog. 2019. PMID: 31242985 Review.
-
Denosumab: a new treatment option for giant cell tumor of bone.Drugs Today (Barc). 2013 Nov;49(11):693-700. doi: 10.1358/dot.2013.49.11.2064725. Drugs Today (Barc). 2013. PMID: 24308016 Review.
Cited by
-
Unusual Presentation of a Giant Cell Tumor of the Bone: A Case Report.Cureus. 2024 Mar 25;16(3):e56929. doi: 10.7759/cureus.56929. eCollection 2024 Mar. Cureus. 2024. PMID: 38665730 Free PMC article.
-
Metformin relieves bone cancer pain by reducing TGFβRI-TRPV1 signaling in rats.Heliyon. 2024 Jul 20;10(15):e34991. doi: 10.1016/j.heliyon.2024.e34991. eCollection 2024 Aug 15. Heliyon. 2024. PMID: 39157315 Free PMC article.
References
-
- Reid R, Banerjee S, Sciot R. Giant cell tumours. In: Fletcher CDM, Unni KK, Mertens F, editors. Pathology and genetics of tumours of soft tissue and bone World Health Organization (WHO) Classification of Tumors. Lyon France: International Agency for Research on Cancer (IARC) Press; 2002. pp. 309–312.
-
- Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am. 2006;37(1):35–51. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
