

Peripheral adenopathies in children - an attempt of clinical morphological profile
- PMID: 34171068
- PMCID: PMC8343490
- DOI: 10.47162/RJME.61.4.21
Peripheral adenopathies in children - an attempt of clinical morphological profile
Abstract
Aim: The authors have proposed to assess peripheral adenopathies in a series of hospitalized children in order to identify and define clinical and morphological profiles of different types of lymph node (LN) diseases.
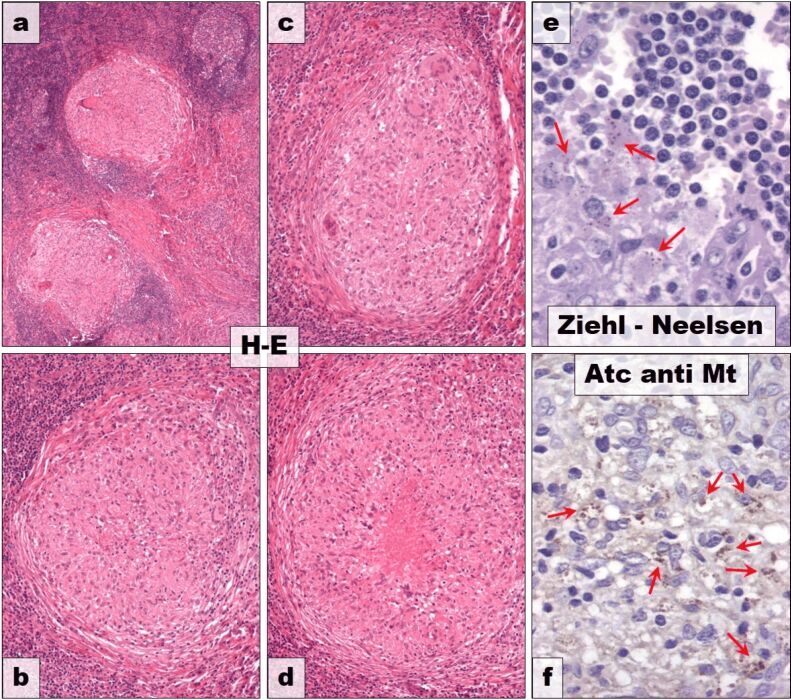
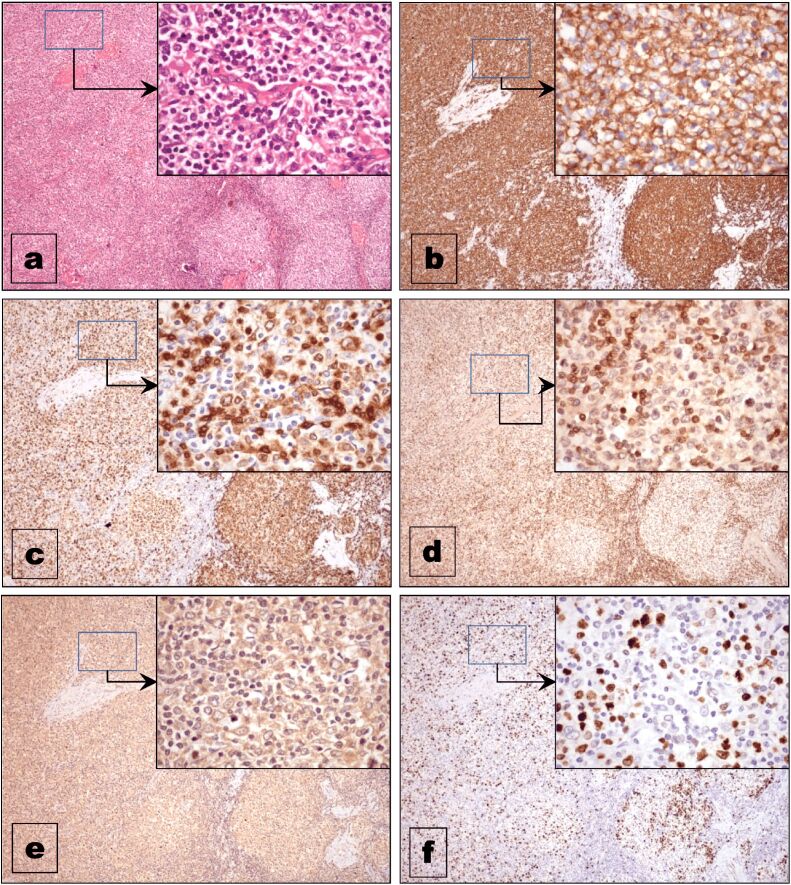
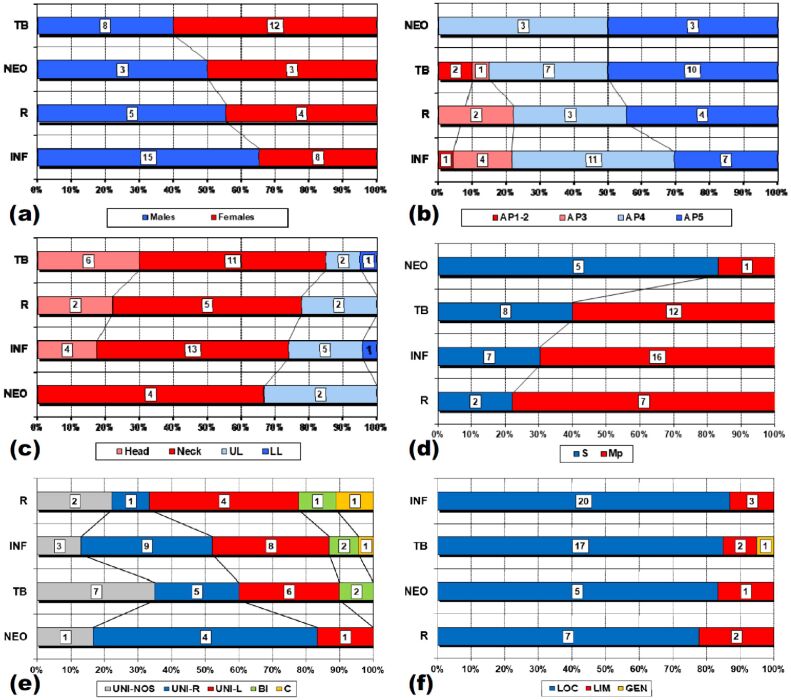
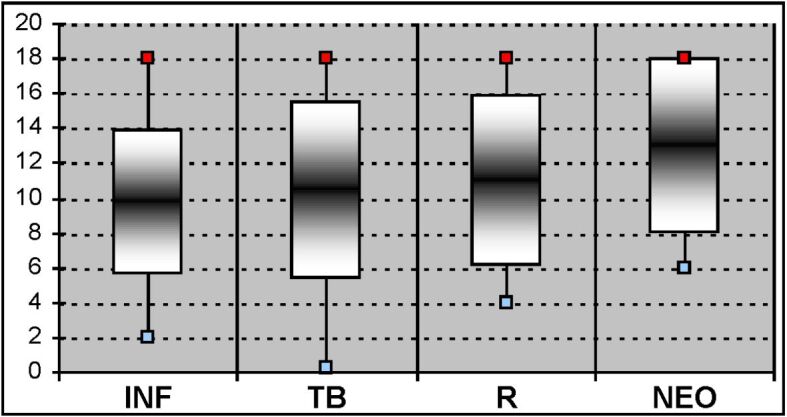
Materials and methods: The studied group consisted of 58 patients less than 18 years of age. The investigation algorithm included: gender, age, site, involvement, side, extension and histopathological (HP) type of LN lesions. Tissue fragments were processed using classical histological techniques (formalin fixation and paraffin embedment) and stained with Hematoxylin-Eosin (HE). In some cases (tuberculous lesions and lymphomas), special stainings (Ziehl-Neelsen) and immunohistochemistry were used. Stratification scales of cases were defined according to each parameter in order to compare the data. All obtained data were assessed individually, compared to each other and with similar data from the literature with the help of a statistical apparatus [χ² (chi-squared) test and analysis of variance (ANOVA) test] in some cases.
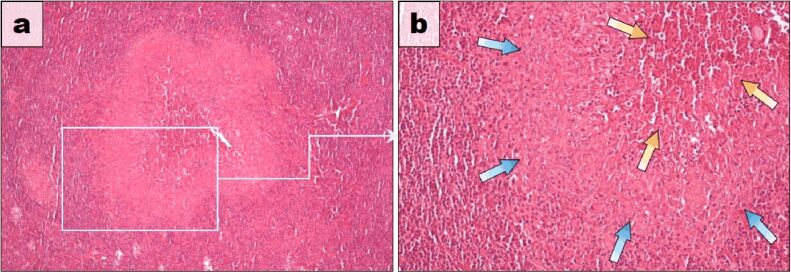
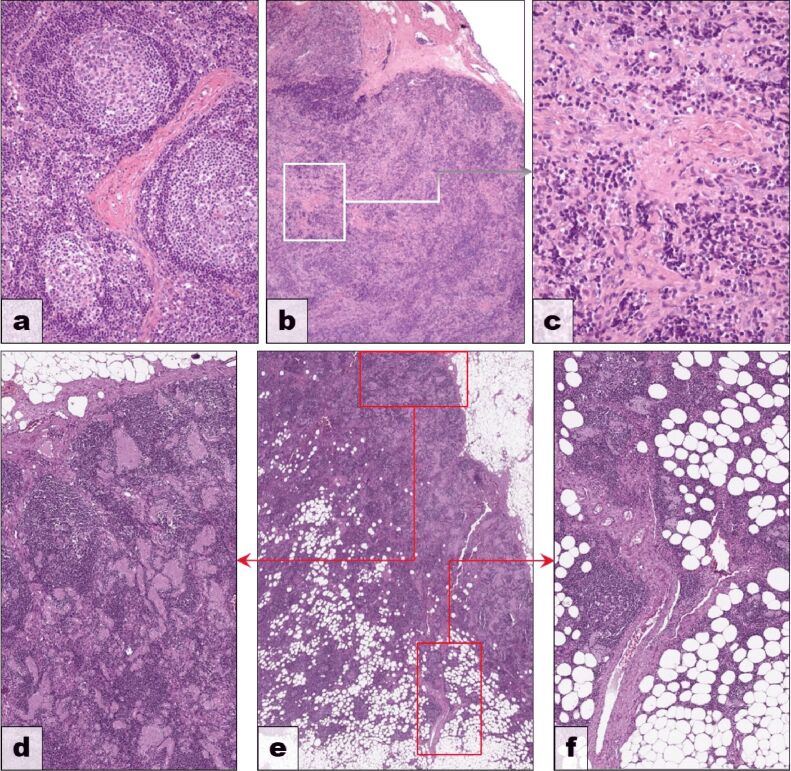
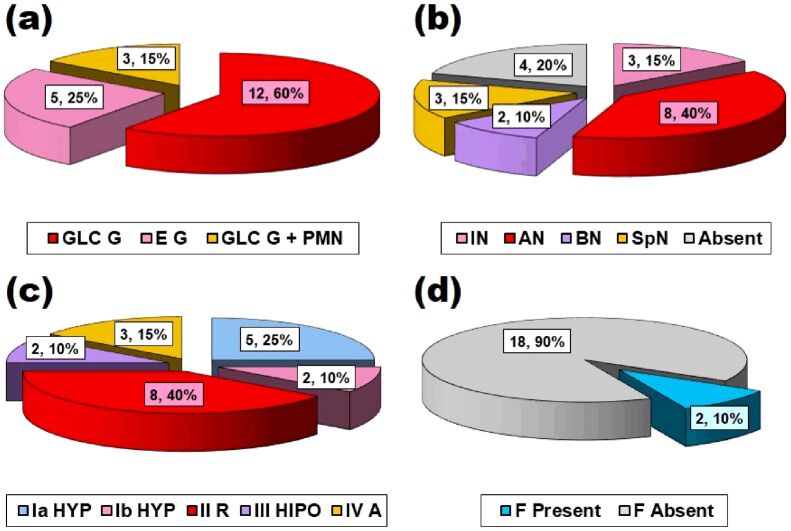
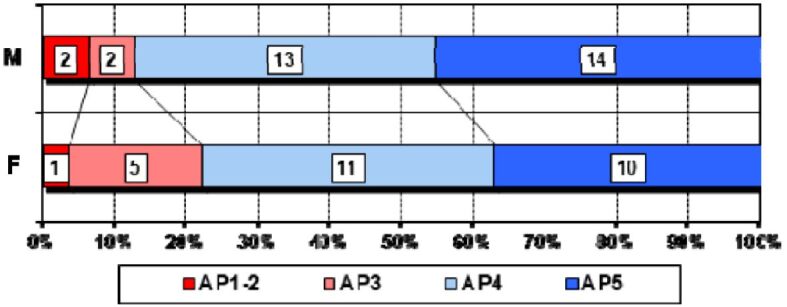
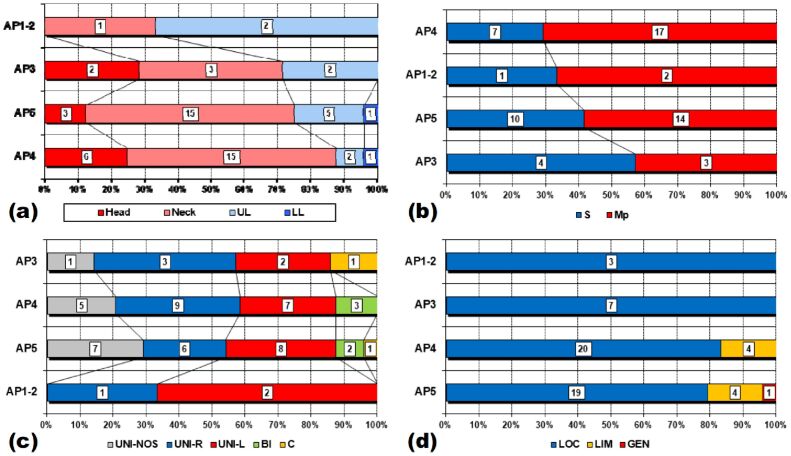
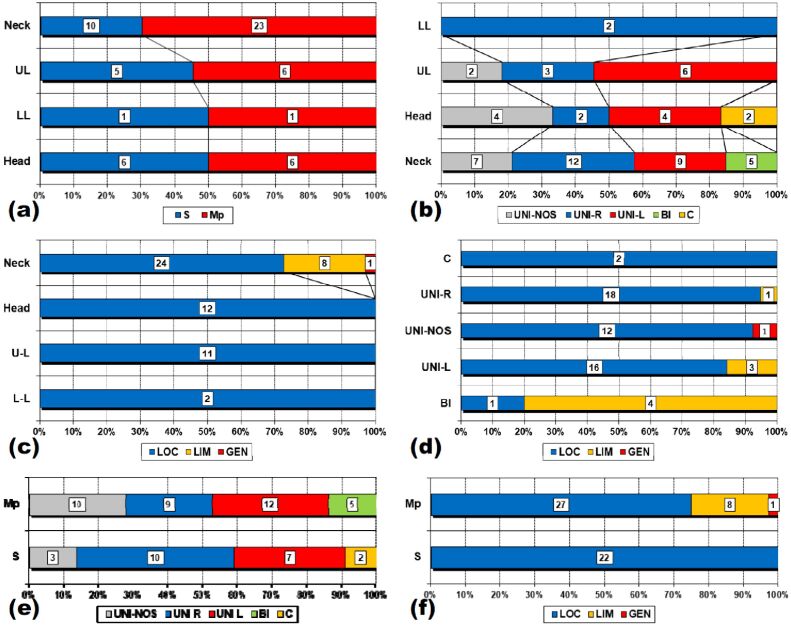
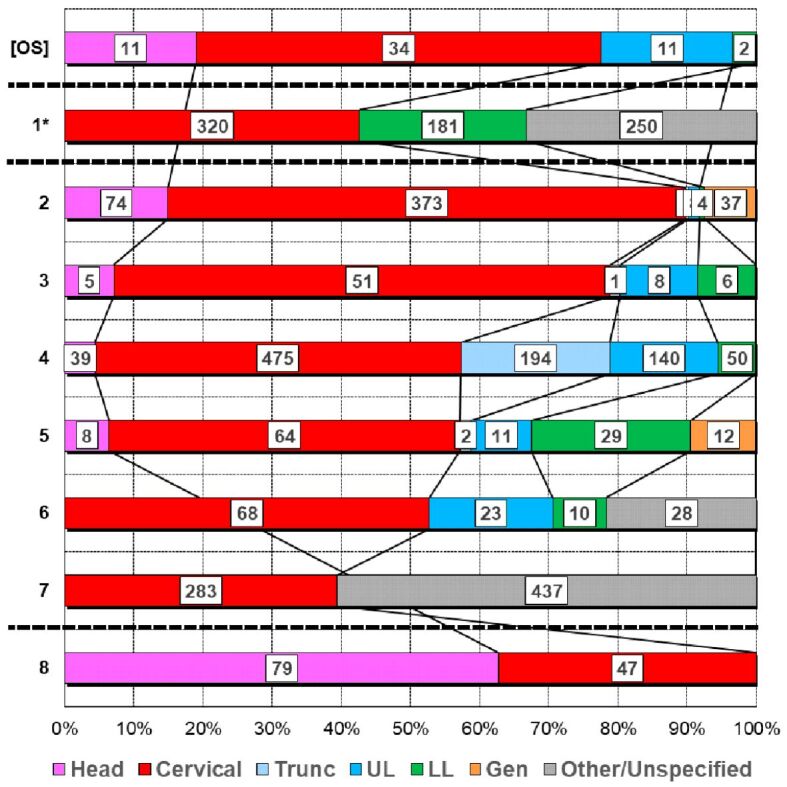
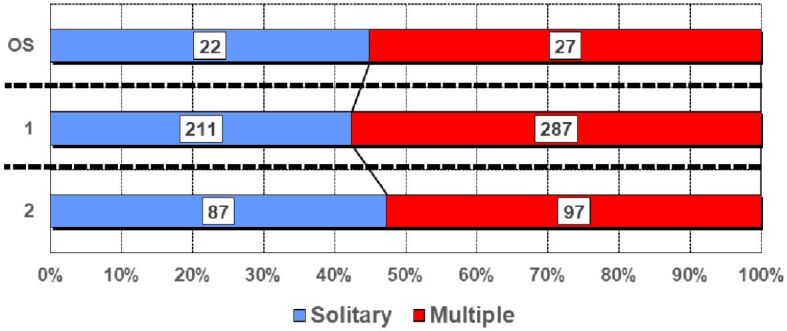
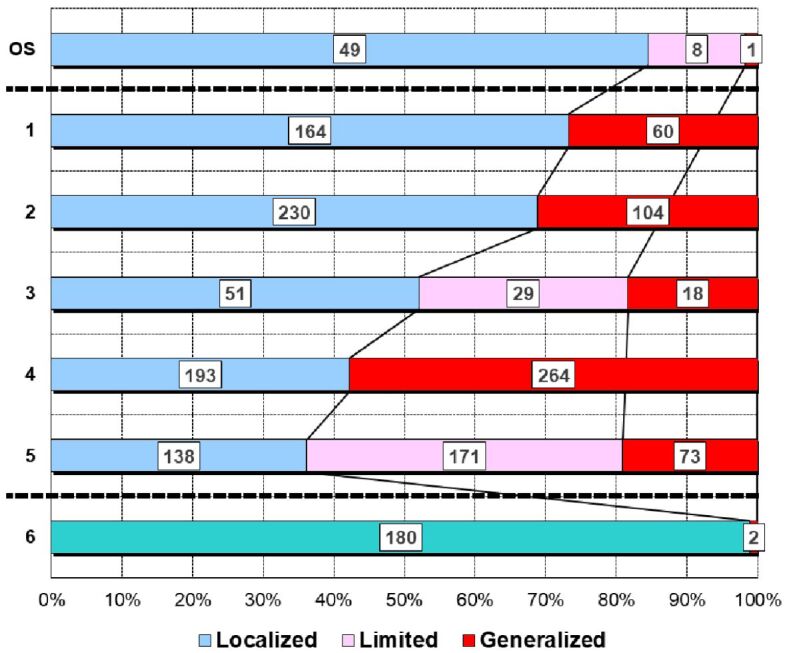
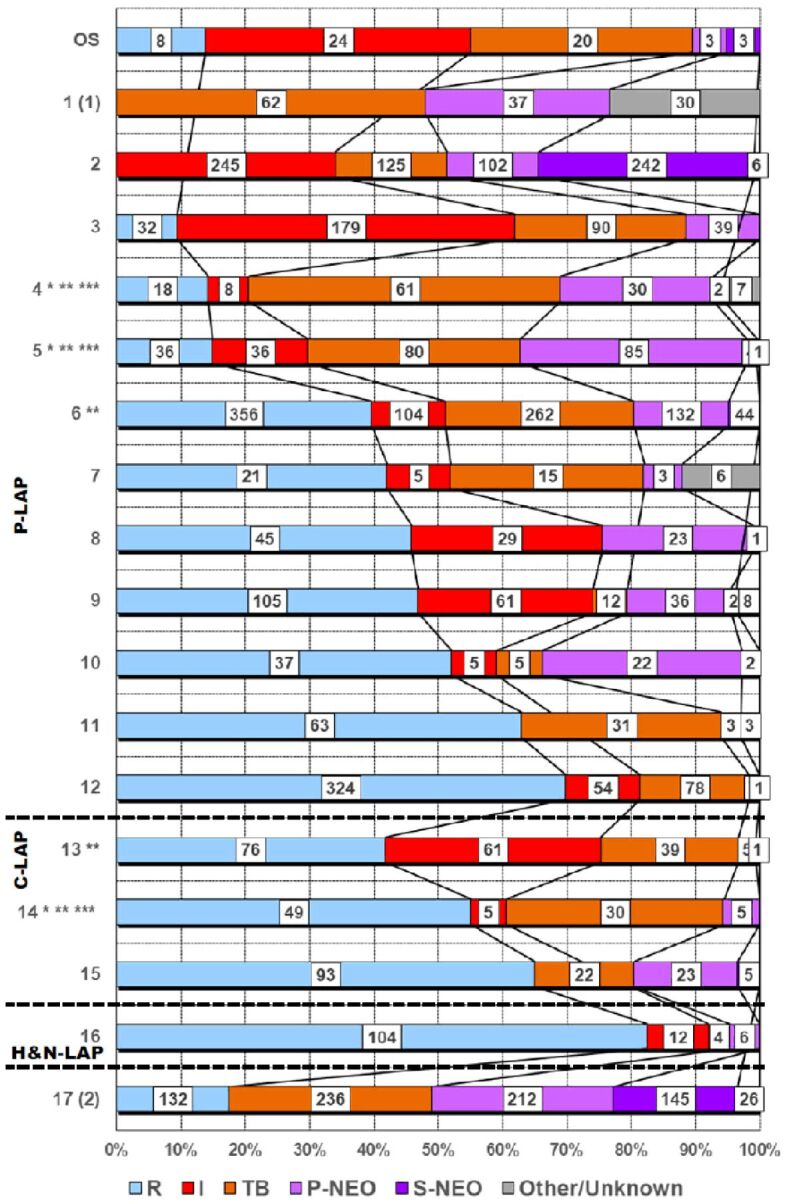
Results: The young patients were slightly more frequently boys, of all ages but with a mean age of 10 and half years. The affected LNs belonged most often to neck region, either on the left or on the right side but sometimes bilateral or even on the midline; usually, more than one LN was involved in the area. In most of the cases, the lesions were localized in only one LN area. HP picture was dominated by the inflammatory processes, firstly the nonspecific ones, followed by tuberculosis.
Discussions: Our observations fitted, for each parameter, with the wide ranges found in the literature. Comparisons between parameters' variations revealed differences, sometimes significant that we tried to organize in clinical and morphological profiles.
Conclusions: The assessment of our data allowed us to define some clinical and morphological profiles of different types of adenopathy that, by improvement on studies including larger series, could be of real use in daily pediatric practice.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures



Similar articles
-
Lymph node tuberculosis - an attempt of clinico-morphological study and review of the literature.Rom J Morphol Embryol. 2014;55(2 Suppl):553-67. Rom J Morphol Embryol. 2014. PMID: 25178325 Review.
-
[Comparative analysis of immunofluorescence double staining for foamy macrophages and Mycobacterium tuberculosis in paraffin-embedded tissue of clinical tuberculous wound].Zhonghua Shao Shang Za Zhi. 2021 Feb 20;37(2):157-163. doi: 10.3760/cma.j.cn501120-20200525-00285. Zhonghua Shao Shang Za Zhi. 2021. PMID: 33498099 Chinese.
-
The clinical-morphological profile of bone and joints tuberculosis - our experience in relation to literature data.Rom J Morphol Embryol. 2017;58(3):887-907. Rom J Morphol Embryol. 2017. PMID: 29250669
-
Clinical-Morphological Aspects in Spinal Tuberculosis.Curr Health Sci J. 2018 Jul-Sep;44(3):250-260. doi: 10.12865/CHSJ.44.03.08. Epub 2018 Jul 15. Curr Health Sci J. 2018. PMID: 30647945 Free PMC article.
-
Morphological aspects in tuberculosis of oral cavity - our experience and a review of the literature attempt.Rom J Morphol Embryol. 2015;56(3):967-87. Rom J Morphol Embryol. 2015. PMID: 26662129 Review.
References
-
- Allhiser JN, McKnight TA, Shank JC. Lymphadenopathy in a family practice. J Fam Pract. 1981;12(1):27–32. - PubMed
-
- Williamson HA. Lymphadenopathy in a family practice: a descriptive study of 249 cases. J Fam Pract. 1985;20(5):449–452. - PubMed
-
- Bazemore AW, Smucker DR. Lymphadenopathy and malignancy. Am Fam Physician. 2002;66(11):2103–2110. - PubMed
-
- Ferrer R. Lymphadenopathy: differential diagnosis and evaluation. Am Fam Physician. 1998;58(6):1313–1320. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
