

Mortality in Escherichia coli bloodstream infections: a multinational population-based cohort study
- PMID: 34172003
- PMCID: PMC8229717
- DOI: 10.1186/s12879-021-06326-x
Mortality in Escherichia coli bloodstream infections: a multinational population-based cohort study
Abstract
Background: Escherichia coli is the most common cause of bloodstream infections (BSIs) and mortality is an important aspect of burden of disease. Using a multinational population-based cohort of E. coli BSIs, our objectives were to evaluate 30-day case fatality risk and mortality rate, and determine factors associated with each.
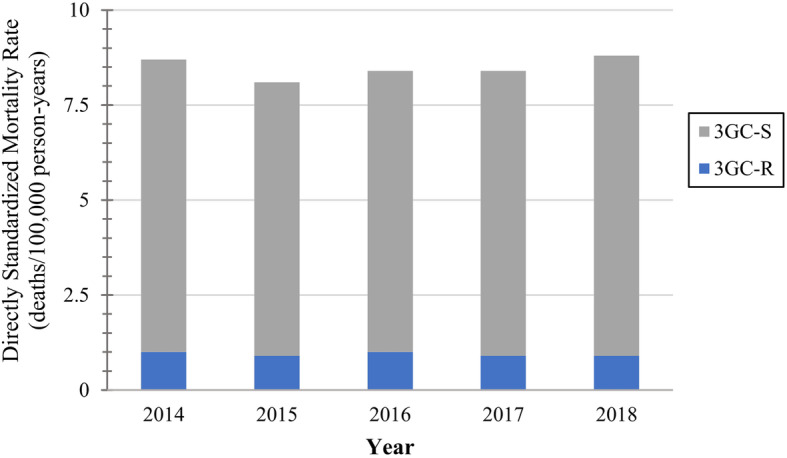
Methods: During 2014-2018, we identified 30-day deaths from all incident E. coli BSIs from surveillance nationally in Finland, and regionally in Sweden (Skaraborg) and Canada (Calgary, Sherbrooke, western interior). We used a multivariable logistic regression model to estimate factors associated with 30-day case fatality risk. The explanatory variables considered for inclusion were year (2014-2018), region (five areas), age (< 70-years-old, ≥70-years-old), sex (female, male), third-generation cephalosporin (3GC) resistance (susceptible, resistant), and location of onset (community-onset, hospital-onset). The European Union 28-country 2018 population was used to directly age and sex standardize mortality rates. We used a multivariable Poisson model to estimate factors associated with mortality rate, and year, region, age and sex were considered for inclusion.
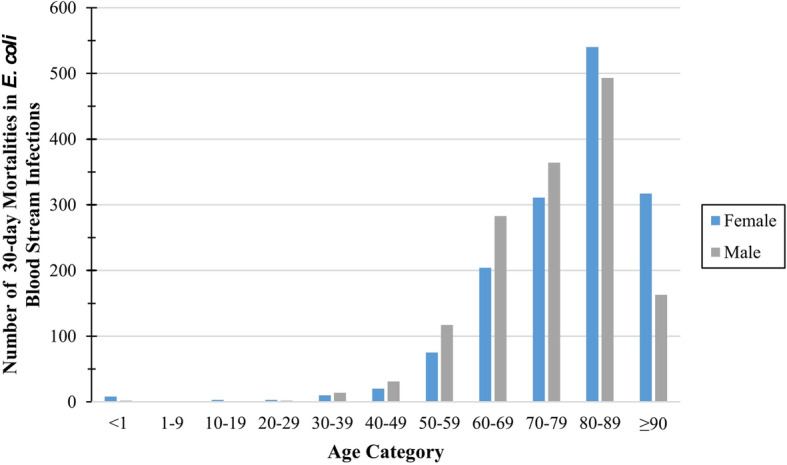
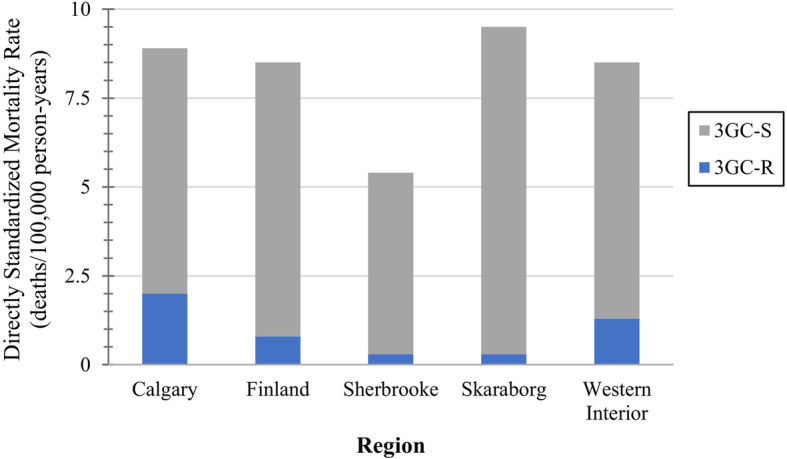
Results: From 38.7 million person-years of surveillance, we identified 2961 30-day deaths in 30,923 incident E. coli BSIs. The overall 30-day case fatality risk was 9.6% (2961/30923). Calgary, Skaraborg, and western interior had significantly increased odds of 30-day mortality compared to Finland. Hospital-onset and 3GC-resistant E. coli BSIs had significantly increased odds of mortality compared to community-onset and 3GC-susceptible. The significant association between age and odds of mortality varied with sex, and contrasts were used to interpret this interaction relationship. The overall standardized 30-day mortality rate was 8.5 deaths/100,000 person-years. Sherbrooke had a significantly lower 30-day mortality rate compared to Finland. Patients that were either ≥70-years-old or male both experienced significantly higher mortality rates than those < 70-years-old or female.
Conclusions: In our study populations, region, age, and sex were significantly associated with both 30-day case fatality risk and mortality rate. Additionally, 3GC resistance and location of onset were significantly associated with 30-day case fatality risk. Escherichia coli BSIs caused a considerable burden of disease from 30-day mortality. When analyzing population-based mortality data, it is important to explore mortality through two lenses, mortality rate and case fatality risk.
Keywords: Bacteremia; Bloodstream infection; Case fatality; Escherichia coli; Mortality; Mortality rate; Population-based.
Conflict of interest statement
MCM reports a scholarship from the Canadian Institutes of Health Research and funding for a Federal Student Work Experience Program placement from the Government of Canada – Genome Research Development Initiative, both related to her PhD program and outside the submitted work. LV reports being a stock holder of Lumed Inc., outside the submitted work. All other authors declare that they have no competing interests.
Figures
References
-
- Nielsen SL, Pedersen C, Jensen TG, Gradel KO, Kolmos HJ, Lassen AT. Decreasing incidence rates of bacteremia: a 9-year population-based study. J Inf Secur. 2014;69(1):51–59. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
