

Limited intestinal inflammation despite diarrhea, fecal viral RNA and SARS-CoV-2-specific IgA in patients with acute COVID-19
- PMID: 34172783
- PMCID: PMC8233421
- DOI: 10.1038/s41598-021-92740-9
Limited intestinal inflammation despite diarrhea, fecal viral RNA and SARS-CoV-2-specific IgA in patients with acute COVID-19
Abstract
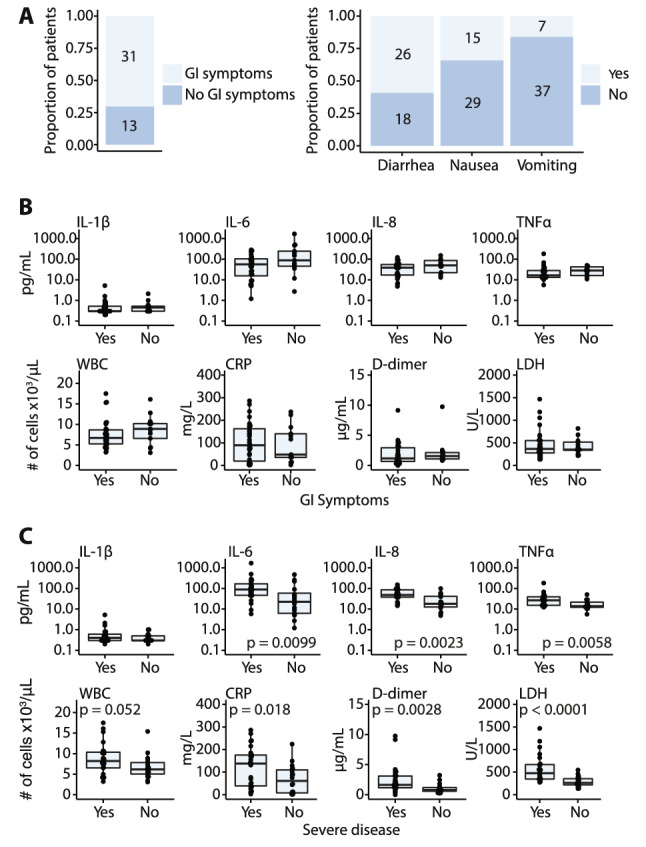
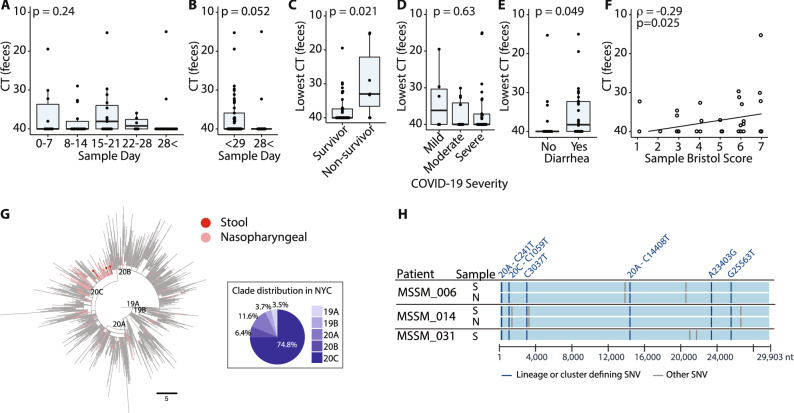
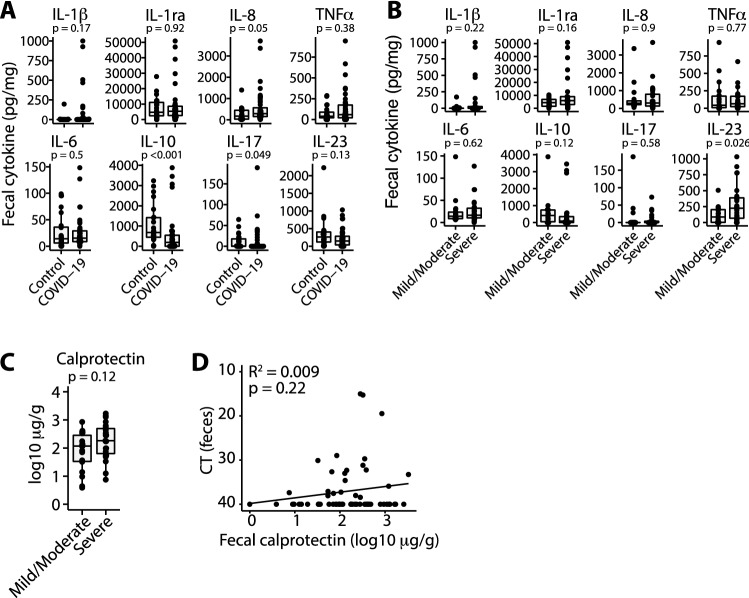
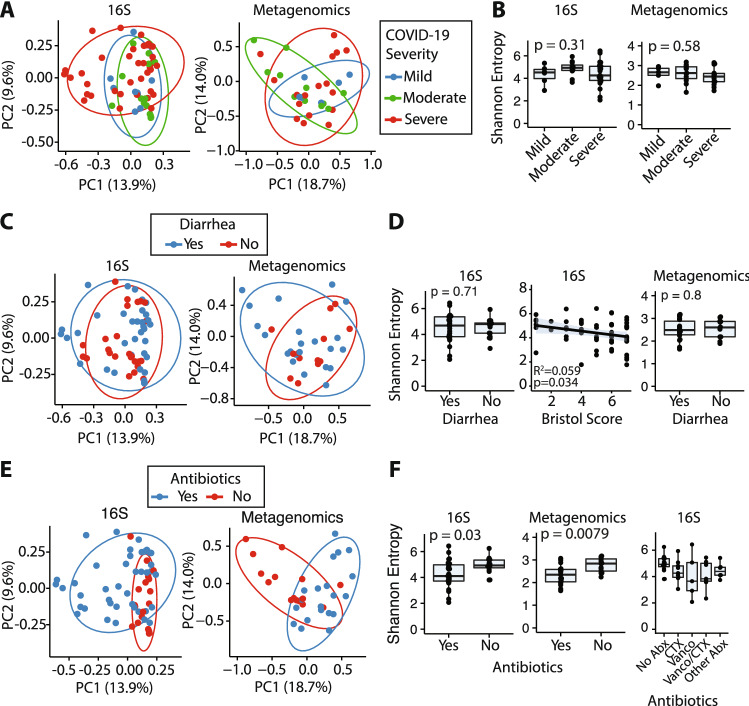
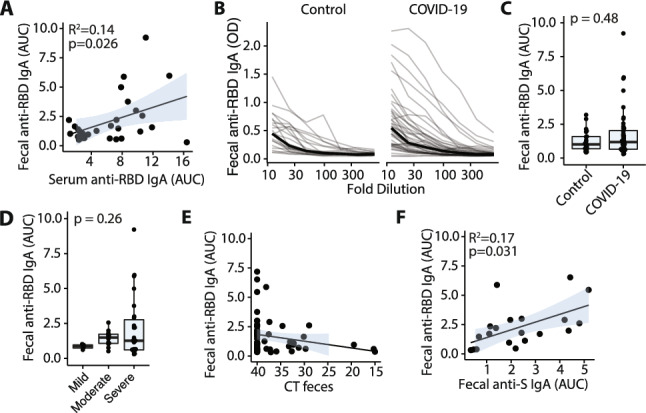
Gastrointestinal symptoms are common in COVID-19 patients but the nature of the gut immune response to SARS-CoV-2 remains poorly characterized, partly due to the difficulty of obtaining biopsy specimens from infected individuals. In lieu of tissue samples, we measured cytokines, inflammatory markers, viral RNA, microbiome composition, and antibody responses in stool samples from a cohort of 44 hospitalized COVID-19 patients. SARS-CoV-2 RNA was detected in stool of 41% of patients and more frequently in patients with diarrhea. Patients who survived had lower fecal viral RNA than those who died. Strains isolated from stool and nasopharynx of an individual were the same. Compared to uninfected controls, COVID-19 patients had higher fecal levels of IL-8 and lower levels of fecal IL-10. Stool IL-23 was higher in patients with more severe COVID-19 disease, and we found evidence of intestinal virus-specific IgA responses associated with more severe disease. We provide evidence for an ongoing humeral immune response to SARS-CoV-2 in the gastrointestinal tract, but little evidence of overt inflammation.
Conflict of interest statement
M.C.D is a consultant for Abbvie, Arena, BMS, Boehringer Ingelheim, Genentech, Janssen, Pfizer, Prometheus Biosciences, Takeda, Target RWE and UCB, has received research support from Janssen, Pfizer, Prometheus Biosciences and Abbvie and is co-founder of Cornerstones Health, Mitest Health, Trellus Health, M.M. is a consultant for Takeda, Genentech, Regeneron, Compugen, Myeloid Therapeutics. F.K. declares that The Icahn School of Medicine at Mount Sinai has filed patent applications regarding SARS-CoV-2 serology assays and has licensed reagents to several commercial entities. J.J.F. serves on the scientific advisor board of Vedanta Biosciences. The remaining authors declare no competing of interest.
Figures
Update of
-
Limited intestinal inflammation despite diarrhea, fecal viral RNA and SARS-CoV-2-specific IgA in patients with acute COVID-19.medRxiv [Preprint]. 2020 Dec 9:2020.09.03.20183947. doi: 10.1101/2020.09.03.20183947. medRxiv. 2020. Update in: Sci Rep. 2021 Jun 25;11(1):13308. doi: 10.1038/s41598-021-92740-9. PMID: 32909002 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 DK123749/DK/NIDDK NIH HHS/United States
- DK112978/DK/NIDDK NIH HHS/United States
- HHSN272201400008C/AI/NIAID NIH HHS/United States
- DK123749/DK/NIDDK NIH HHS/United States
- T32 AI007605/AI/NIAID NIH HHS/United States
- R01 DK112978/DK/NIDDK NIH HHS/United States
- R01 DK124133/DK/NIDDK NIH HHS/United States
- S10 OD018522/OD/NIH HHS/United States
- S10 OD026880/OD/NIH HHS/United States
- R01 GM108505/GM/NIGMS NIH HHS/United States
- 5T32AI007605/NH/NIH HHS/United States
- GM108505/NH/NIH HHS/United States
- 75N93019C00051/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
