

Fully automated analysis combining [18F]-FET-PET and multiparametric MRI including DSC perfusion and APTw imaging: a promising tool for objective evaluation of glioma progression
- PMID: 34173008
- PMCID: PMC8566389
- DOI: 10.1007/s00259-021-05427-8
Fully automated analysis combining [18F]-FET-PET and multiparametric MRI including DSC perfusion and APTw imaging: a promising tool for objective evaluation of glioma progression
Abstract
Purpose: To evaluate diagnostic accuracy of fully automated analysis of multimodal imaging data using [18F]-FET-PET and MRI (including amide proton transfer-weighted (APTw) imaging and dynamic-susceptibility-contrast (DSC) perfusion) in differentiation of tumor progression from treatment-related changes in patients with glioma.
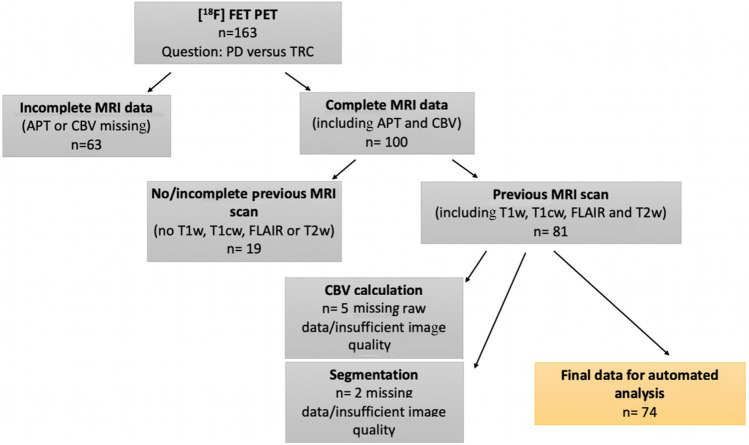
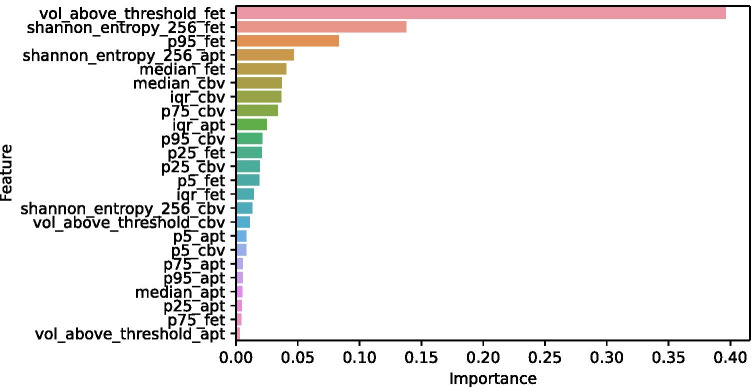
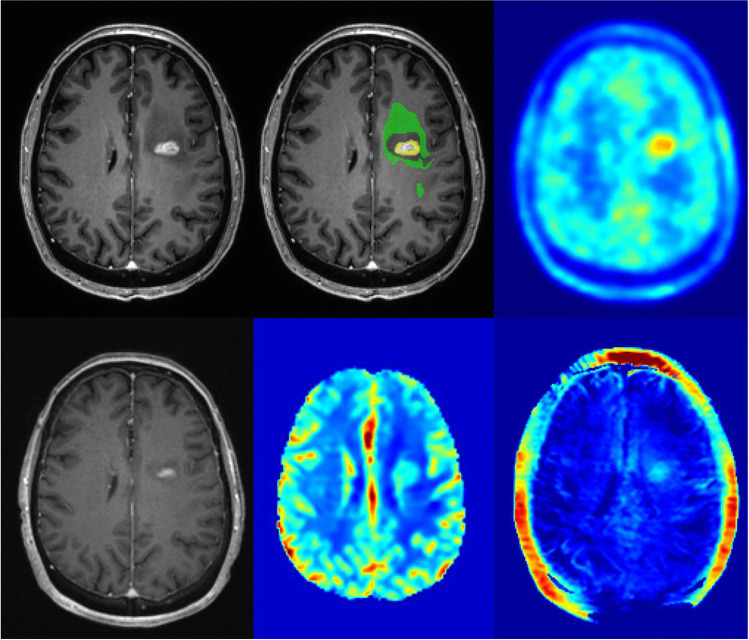
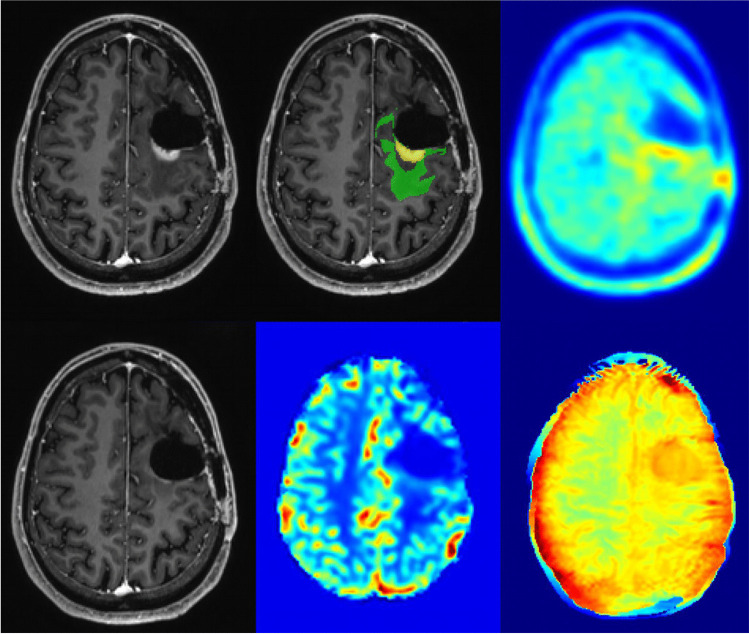
Material and methods: At suspected tumor progression, MRI and [18F]-FET-PET data as part of a retrospective analysis of an observational cohort of 66 patients/74 scans (51 glioblastoma and 23 lower-grade-glioma, 8 patients included at two different time points) were automatically segmented into necrosis, FLAIR-hyperintense, and contrast-enhancing areas using an ensemble of deep learning algorithms. In parallel, previous MR exam was processed in a similar way to subtract preexisting tumor areas and focus on progressive tumor only. Within these progressive areas, intensity statistics were automatically extracted from [18F]-FET-PET, APTw, and DSC-derived cerebral-blood-volume (CBV) maps and used to train a Random Forest classifier with threefold cross-validation. To evaluate contribution of the imaging modalities to the classifier's performance, impurity-based importance measures were collected. Classifier performance was compared with radiology reports and interdisciplinary tumor board assessments.
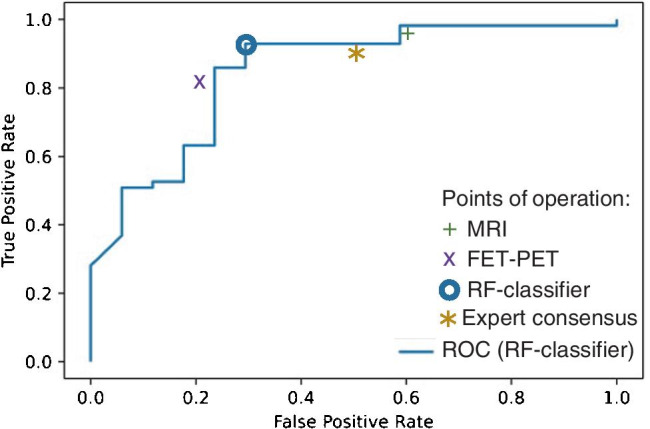
Results: In 57/74 cases (77%), tumor progression was confirmed histopathologically (39 cases) or via follow-up imaging (18 cases), while remaining 17 cases were diagnosed as treatment-related changes. The classification accuracy of the Random Forest classifier was 0.86, 95% CI 0.77-0.93 (sensitivity 0.91, 95% CI 0.81-0.97; specificity 0.71, 95% CI 0.44-0.9), significantly above the no-information rate of 0.77 (p = 0.03), and higher compared to an accuracy of 0.82 for MRI (95% CI 0.72-0.9), 0.81 for [18F]-FET-PET (95% CI 0.7-0.89), and 0.81 for expert consensus (95% CI 0.7-0.89), although these differences were not statistically significant (p > 0.1 for all comparisons, McNemar test). [18F]-FET-PET hot-spot volume was single-most important variable, with relevant contribution from all imaging modalities.
Conclusion: Automated, joint image analysis of [18F]-FET-PET and advanced MR imaging techniques APTw and DSC perfusion is a promising tool for objective response assessment in gliomas.
Keywords: APTw; B. coshared last; DSC perfusion; Fully automated; Glioma progression; J. S. and Wiestler; Kirschke; Multiparametric MRI; [18F]-FET-PET.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Chu HH, Choi SH, Ryoo I, Kim SC, Yeom JA, Shin H, et al. Differentiation of true progression from pseudoprogression in glioblastoma treated with radiation therapy and concomitant temozolomide: comparison study of standard and high-b-value diffusion-weighted imaging. Radiology. 2013;269:831–840. doi: 10.1148/radiol.13122024. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
