

Efficacy and safety of flexible versus rigid endoscopic third ventriculostomy in pediatric and adult populations: a systematic review and meta-analysis
- PMID: 34173114
- PMCID: PMC8827229
- DOI: 10.1007/s10143-021-01590-6
Efficacy and safety of flexible versus rigid endoscopic third ventriculostomy in pediatric and adult populations: a systematic review and meta-analysis
Abstract
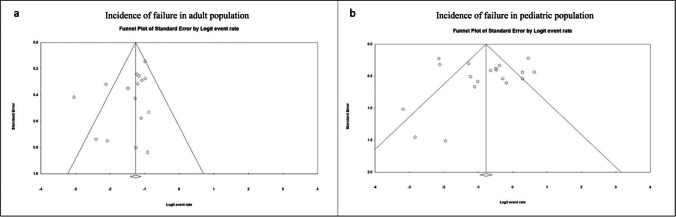
Endoscopic third ventriculostomy (ETV) is a well-established surgical procedure for hydrocephalus treatment, but there is sparse evidence on the optimal choice between flexible and rigid approaches. A meta-analysis was conducted to compare efficacy and safety profiles of both techniques in pediatrics and adults. A comprehensive search was conducted on PubMED, EMBASE, and Cochrane until 11/10/2019. Efficacy was evaluated comparing incidence of ETV failure, while safety was defined by the incidence of perioperative complications, intraoperative bleedings, and deaths. Random-effects models were used to pool the incidence. Out of 1365 studies, 46 case series were meta-analyzed, yielding 821 patients who underwent flexible ETV and 2918 who underwent rigid ETV, with an age range of [5 days-87 years]. Although flexible ETV had a higher incidence of failure in adults (flexible: 54%, 95%CI: 22-82% vs rigid: 20%, 95%CI: 22-82%) possibly due to confounding due to etiology in adults treated with flexible, a smaller difference was seen in pediatrics (flexible: 36%, pediatric: 32%). Safety profiles were acceptable for both techniques, with a certain degree of variability for complications (flexible 2%, rigid 18%) and death (flexible 1%, rigid 3%) in pediatrics as well as complications (rigid 9%, flexible 13%), death (flexible 4%, rigid 6%) and intra-operative bleeding events (rigid 6%, flexible 8%) in adults. No clear superiority in efficacy could be depicted between flexible and rigid ETV for hydrocephalus treatment. Safety profiles varied by age but were acceptable for both techniques. Well-designed comparative studies are needed to assess the optimal endoscopic treatment option for hydrocephalus.
Keywords: Complications; Efficacy; Endoscopic third ventriculostomy; Flexible neuroendoscopy; Hydrocephalus; Rigid neuroendoscopy.
© 2021. The Author(s).
Conflict of interest statement
No conflict of interest or competing interests to report related to this work.
Figures




References
-
- Abbassy M, Aref K, Farhoud A, Hekal A. (2018) Outcome of single-trajectory rigid endoscopic third ventriculostomy and biopsy in the management algorithm of pineal region tumors: a case series and review of the literature. Childs Nerv Syst. 1–10. - PubMed
-
- Ali M, Usman M, Khan Z, et al. Endoscopic third ventriculostomy for obstructive hydrocephalus. J Coll Physicians Surg Pak. 2013;23(5):338–341. - PubMed
-
- Aref M, Martyniuk A, Nath S, et al. Endoscopic Third Ventriculostomy: Outcome Analysis of an Anterior Entry Point. World Neurosurg. 2017;104:554–559. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
