

Telephone follow-up to reduce unplanned hospital returns for older emergency department patients: A randomized trial
- PMID: 34173229
- PMCID: PMC9290482
- DOI: 10.1111/jgs.17336
Telephone follow-up to reduce unplanned hospital returns for older emergency department patients: A randomized trial
Abstract
Background/objectives: Telephone follow-up calls could optimize the transition from the emergency department (ED) to home for older patients. However, the effects on hospital return rates are not clear. We investigated whether telephone follow-up reduces unplanned hospitalizations and/or unplanned ED return visits within 30 days of ED discharge.
Design: Pragmatic randomized controlled trial with allocation by month; odd months intervention group, even months control group.
Setting: Two ED locations of a non-academic teaching hospital in The Netherlands.
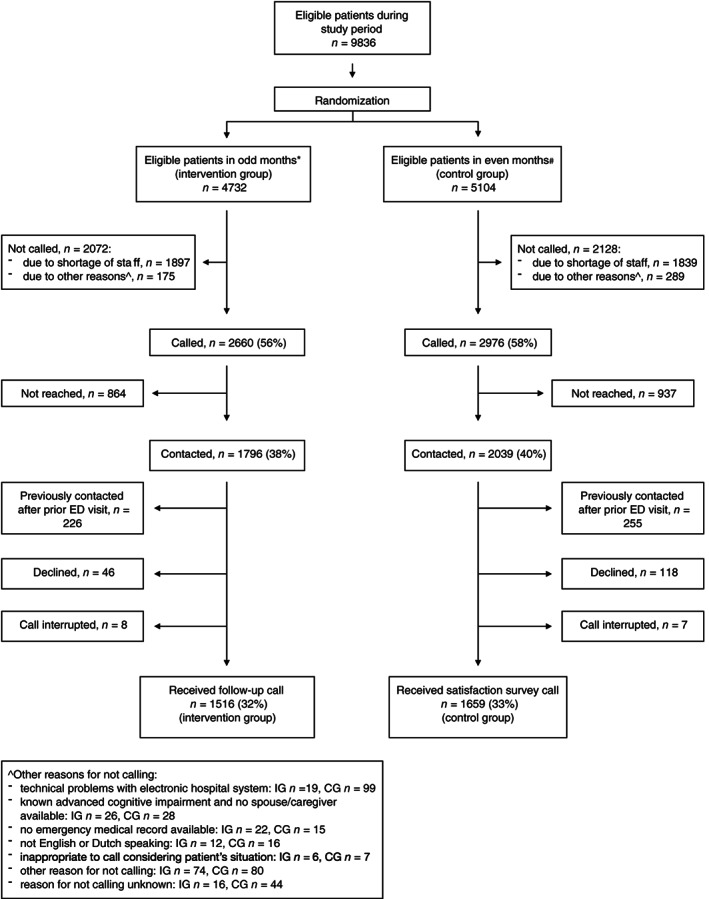
Participants: Community-dwelling adults aged ≥70 years, discharged home from the ED were randomized to the intervention group (N = 4732) or control group (N = 5104).
Intervention: Intervention group patients: semi-scripted telephone call from an ED nurse within 24 h after discharge to identify post-discharge problems and review discharge instructions. Control group patients: scripted satisfaction survey telephone call.
Measurements: Primary outcome: total number of unplanned hospitalizations and/or ED return visits within 30 days of ED discharge.
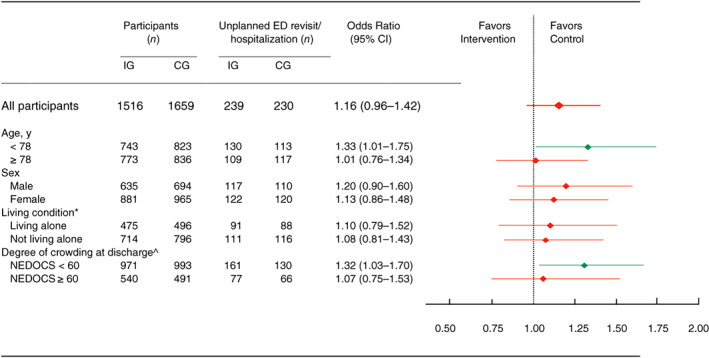
Secondary outcomes: separate numbers of unplanned hospitalizations and ED return visits. Subgroup analysis by age, sex, living condition, and degree of crowding in the ED at discharge.
Results: Overall, 42% were males, and median age was 78 years. In the intervention group, 1516 of 4732 patients (32%) consented, and in the control group 1659 of 5104 (33%) patients. Unplanned 30-day hospitalization and/or ED return visit was found in 16% of intervention group patients and 14% of control group patients (odds ratio 1.16; 95% confidence interval: 0.96-1.42). Also, no statistically significant differences were found in secondary outcome measures. Within the subgroups, the intervention did not have beneficial effects for the intervention group.
Conclusion: Telephone follow-up after ED discharge in older patients did not result in reduction of unplanned hospital admissions and/or ED return visits within 30 days. These results raise the question of whether other outcomes could be improved by post-discharge ED telephone follow-up.
Keywords: emergency department; geriatric; older patients; post-discharge follow-up; telephone.
© 2021 The Authors. Journal of the American Geriatrics Society published by Wiley Periodicals LLC on behalf of The American Geriatrics Society.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Telephone Follow-Up for Older Adults Discharged to Home from the Emergency Department: A Pragmatic Randomized Controlled Trial.J Am Geriatr Soc. 2018 Mar;66(3):452-458. doi: 10.1111/jgs.15142. Epub 2017 Dec 22. J Am Geriatr Soc. 2018. PMID: 29272029 Clinical Trial.
-
A randomized trial exploring the effect of a telephone call follow-up on care plan compliance among older adults discharged home from the emergency department.Acad Emerg Med. 2014 Feb;21(2):188-95. doi: 10.1111/acem.12308. Acad Emerg Med. 2014. PMID: 24673675 Clinical Trial.
-
Supporting at-risk older adults transitioning from hospital to home: who benefits from an evidence-based patient-centered discharge planning intervention? Post-hoc analysis from a randomized trial.BMC Geriatr. 2020 Mar 2;20(1):84. doi: 10.1186/s12877-020-1494-3. BMC Geriatr. 2020. PMID: 32122311 Free PMC article. Clinical Trial.
-
The effect of a telephone follow-up call for older patients, discharged home from the emergency department on health-related outcomes: a systematic review of controlled studies.Int J Emerg Med. 2021 Feb 18;14(1):13. doi: 10.1186/s12245-021-00336-x. Int J Emerg Med. 2021. PMID: 33602115 Free PMC article. Review.
-
Emergency Department Interventions for Older Adults: A Systematic Review.J Am Geriatr Soc. 2019 Jul;67(7):1516-1525. doi: 10.1111/jgs.15854. Epub 2019 Mar 15. J Am Geriatr Soc. 2019. PMID: 30875098 Free PMC article.
Cited by
-
Critical revisits after discharge from the emergency department.Int J Emerg Med. 2025 Mar 3;18(1):41. doi: 10.1186/s12245-025-00847-x. Int J Emerg Med. 2025. PMID: 40033175 Free PMC article.
-
A mapping review of interventions to address patients who frequently seek care in the emergency department.BMC Emerg Med. 2024 Mar 27;24(1):49. doi: 10.1186/s12873-024-00970-7. BMC Emerg Med. 2024. PMID: 38539107 Free PMC article.
-
Investigating patient engagement associations between a postdischarge texting programme and patient experience, readmission and revisit rates outcomes.BMJ Open. 2024 Mar 13;14(3):e079775. doi: 10.1136/bmjopen-2023-079775. BMJ Open. 2024. PMID: 38485169 Free PMC article.
-
ChatGPT's Role in Improving Education Among Patients Seeking Emergency Medical Treatment.West J Emerg Med. 2024 Sep;25(5):845-855. doi: 10.5811/westjem.18650. West J Emerg Med. 2024. PMID: 39319818 Free PMC article.
-
Access to the internet and mobile applications in a mixed population emergency department: A repeated cross-sectional survey.PEC Innov. 2024 Sep 12;5:100340. doi: 10.1016/j.pecinn.2024.100340. eCollection 2024 Dec 15. PEC Innov. 2024. PMID: 39314544 Free PMC article.
References
-
- Aminzadeh F, Dalziel WB. Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med. 2002;39:238‐247. - PubMed
-
- Arendts G, Fitzhardinge S, Pronk K, Hutton M, Nagree Y, Donaldson M. Derivation of a nomogram to estimate probability of revisit in at‐risk older adults discharged from the emergency department. Intern Emerg Med. 2013;8:249‐254. - PubMed
-
- de Gelder J, Lucke JA, de Groot B, et al. Predictors and outcomes of revisits in older adults discharged from the emergency department. J Am Geriatr Soc. 2018;66:735‐741. - PubMed
-
- Biese KJ, Busby‐Whitehead J, Cai J, et al. Telephone follow‐up for older adults discharged to home from the emergency department: a pragmatic randomized controlled trial. J Am Geriatr Soc. 2018;66:452‐458. - PubMed
-
- Caplan GA, Brown A, Croker WD, Doolan J. Risk of admission within 4 weeks of discharge of elderly patients from the emergency department—the DEED study. Discharge of elderly from emergency department. Age Ageing. 1998;27:697‐702. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
