

The impact of a national COVID-19 lockdown on acute coronary syndrome hospitalisations in New Zealand (ANZACS-QI 55)
- PMID: 34173604
- PMCID: PMC7677076
- DOI: 10.1016/j.lanwpc.2020.100056
The impact of a national COVID-19 lockdown on acute coronary syndrome hospitalisations in New Zealand (ANZACS-QI 55)
Abstract
Background: Countries with a high incidence of coronavirus 2019 (COVID-19) reported reduced hospitalisations for acute coronary syndromes (ACS) during the pandemic. This study describes the impact of a nationwide lockdown on ACS hospitalisations in New Zealand (NZ), a country with a low incidence of COVID-19.
Methods: All patients admitted to a NZ Hospital with ACS who underwent coronary angiography in the All NZ ACS Quality Improvement registry during the lockdown (23 March - 26 April 2020) were compared with equivalent weeks in 2015-2019. Ambulance attendances and regional community troponin-I testing were compared for lockdown and non-lockdown (1 July 2019 to 16 February 2020) periods.
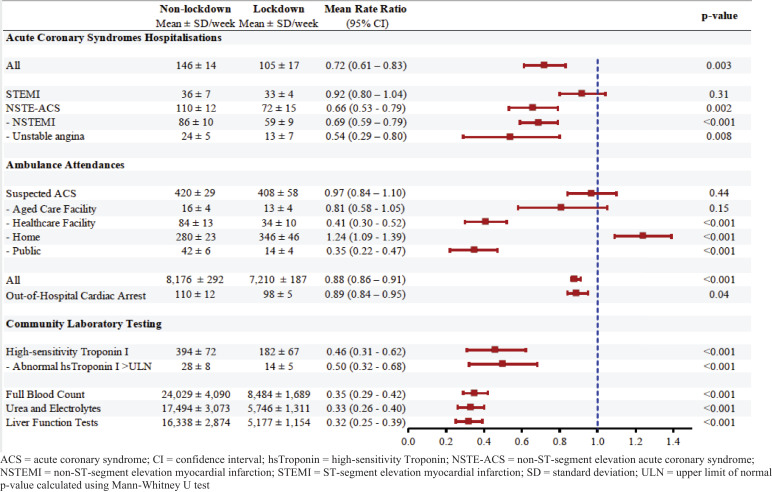
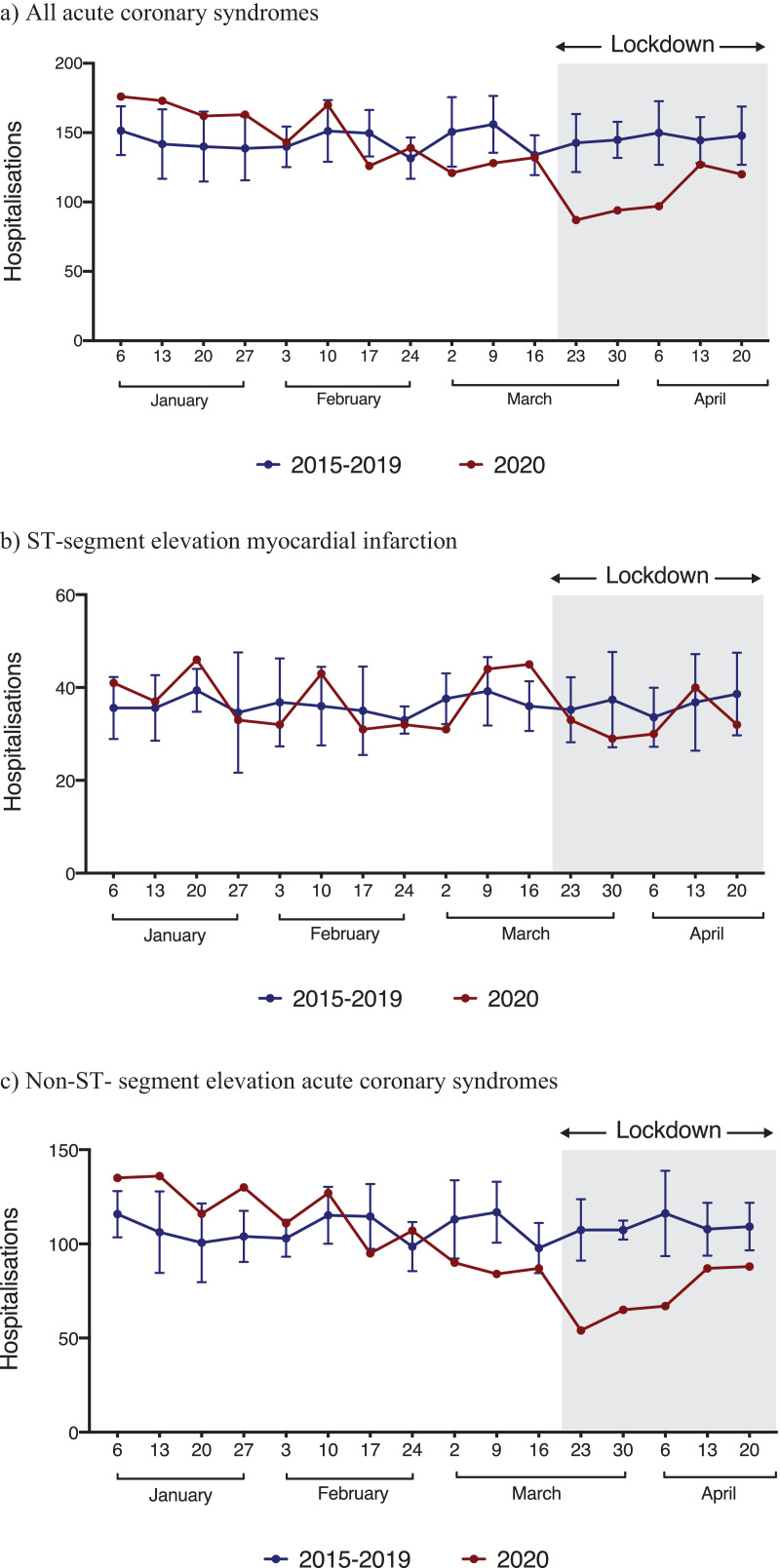
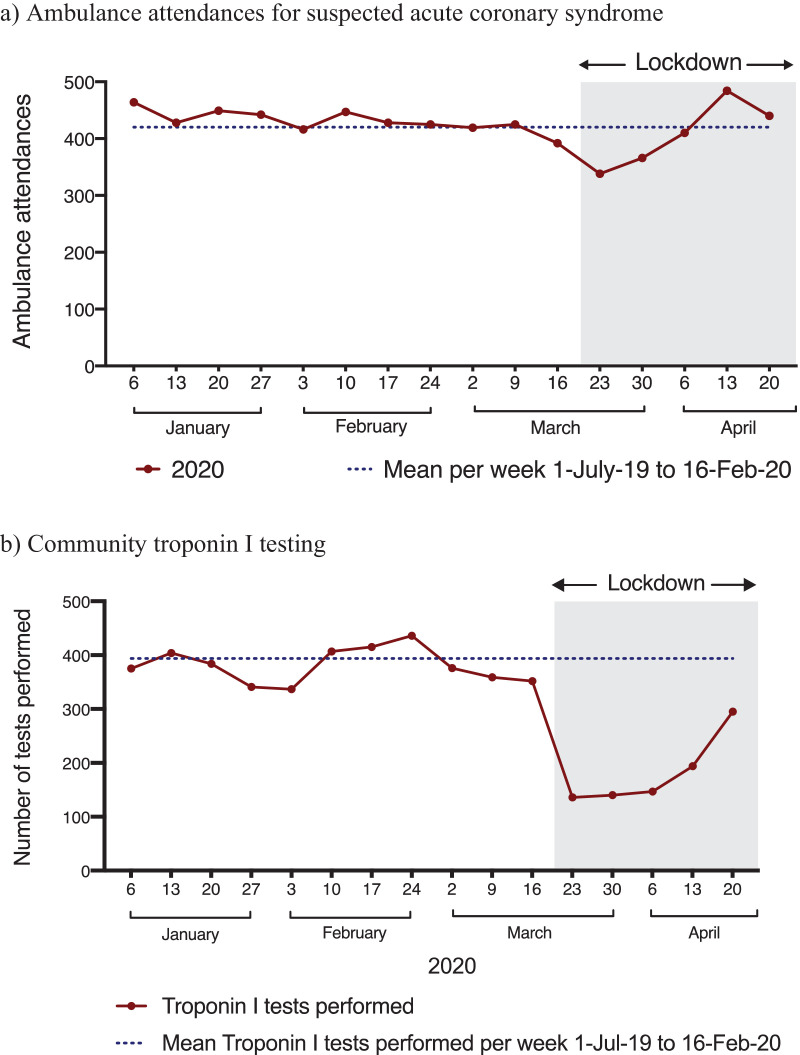
Findings: Hospitalisation for ACS was lower during the 5-week lockdown (105 vs. 146 per-week, rate ratio 0•72 [95% CI 0•61-0•83], p = 0.003). This was explained by fewer admissions for non-ST-segment elevation ACS (NSTE-ACS; p = 0•002) but not ST-segment elevation myocardial infarction (STEMI; p = 0•31). Patient characteristics and in-hospital mortality were similar. For STEMI, door-to-balloon times were similar (70 vs. 72 min, p = 0•52). For NSTE-ACS, there was an increase in percutaneous revascularisation (59% vs. 49%, p<0•001) and reduction in surgical revascularisation (9% vs. 15%, p = 0•005). There were fewer ambulance attendances for cardiac arrests (98 vs. 110 per-week, p = 0•04) but no difference for suspected ACS (408 vs. 420 per-week, p = 0•44). Community troponin testing was lower throughout the lockdown (182 vs. 394 per-week, p<0•001).
Interpretation: Despite the low incidence of COVID-19, there was a nationwide decrease in ACS hospitalisations during the lockdown. These findings have important implications for future pandemic planning.
Funding: The ANZACS-QI registry receives funding from the New Zealand Ministry of Health.
Keywords: Acute coronary syndrome; Coronavirus 2019.
© 2020 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
DZC is supported by the A.H. Couch Research Fellowship. PDA is supported by a Heart Foundation of New Zealand Senior Fellowship (1844). YBL is supported by the Middlemore Cardiac Trust. HDW has received grant support paid to the institution and fees for serving on Steering Committees of the ODYSSEY trial from Sanofi and Regeneron Pharmaceuticals, of the STRENGTH trial from Omthera Pharmaceuticals, and of the HEART-FID study from American Regent, of the CAMELLIA study from Eisai Inc., of the DAL-GENE study from DalCor Pharma UK Inc., of the AEGIS-II study from CSL Behring, of the SCORED and SOLOIST-WHF trials from Sanofi Australia Pty Ltd., and of the CLEAR OUTCOMES study from Esperion Therapeutics Inc., and of the ACCELERATE study from Eli Lilly and Company. He has been on an Advisory Board for Genentech, Inc. San Francisco. He has received interview fees paid at ACC2018 Cardiovascular Forum by AstraZeneca.
Figures
References
-
- Roser M., Ritchie H., Ortiz-Ospina E., Hasell J. Coronavirus pandemic (COVID-19) 2020 [27th April 2020]. Available from: https://ourworldindata.org/coronavirus.
LinkOut - more resources
Full Text Sources
Miscellaneous
