

Influence of socioeconomic deprivation on interventions and outcomes for patients admitted with COVID-19 to critical care units in Scotland: A national cohort study
- PMID: 34173618
- PMCID: PMC7834626
- DOI: 10.1016/j.lanepe.2020.100005
Influence of socioeconomic deprivation on interventions and outcomes for patients admitted with COVID-19 to critical care units in Scotland: A national cohort study
Abstract
Background: Coronavirus disease 2019 (COVID-19) can lead to significant respiratory failure with between 14% and 18% of hospitalised patients requiring critical care admission. This study describes the impact of socioeconomic deprivation on 30-day survival following critical care admission for COVID-19, and the impact of the COVID-19 pandemic on critical care capacity in Scotland.
Methods: This cohort study used linked national hospital records including ICU, virology testing and national death records to identify and describe patients with COVID-19 admitted to critical care units in Scotland. Multivariable logistic regression was used to assess the impact of deprivation on 30-day mortality. Critical care capacity was described by reporting the percentage of baseline ICU bed utilisation required.
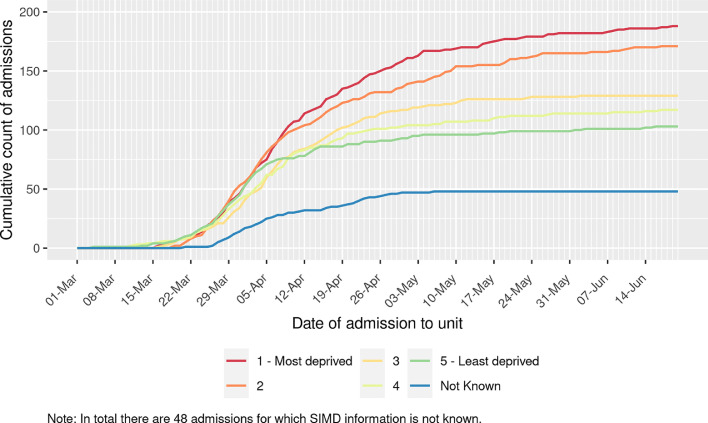
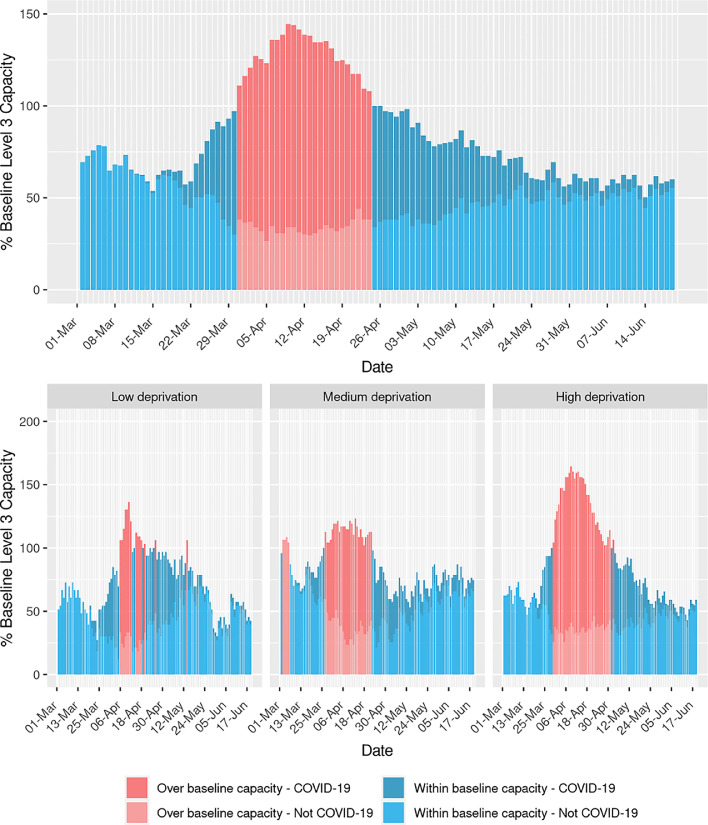
Findings: There were 735 patients with COVID-19 admitted to critical care units across Scotland from 1/3/2020 to 20/6/2020. There was a higher proportion of patients from more deprived areas, with 183 admissions (24.9%) from the most deprived quintile and 100 (13.6%) from the least deprived quintile. Overall, 30-day mortality was 34.8%. After adjusting for age, sex and ethnicity, mortality was significantly higher in patients from the most deprived quintile (OR 1.97, 95%CI 1.13, 3.41, p=0.016). ICUs serving populations with higher levels of deprivation spent a greater amount of time over their baseline ICU bed capacity.
Interpretation: Patients with COVID-19 living in areas with greatest socioeconomic deprivation had a higher frequency of critical care admission and a higher adjusted 30-day mortality. ICUs in health boards with higher levels of socioeconomic deprivation had both higher peak occupancy and longer duration of occupancy over normal maximum capacity.
Funding: None.
Keywords: COVID-19; Intensive care; Mortality; Social deprivation.
© 2020 The Authors.
Conflict of interest statement
All authors declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; NL is Director of Research, Intensive Care Society; JM is funded by a THIS.Institute (University of Cambridge) Research Fellowship (PD-2019-02-16). The funder had no role in the study design; in the collection, analysis and interpretation of the data; in the writing of the report; and in the decision to submit the paper for publication.
Figures
References
-
- UK Government (2020) Coronavirus (COVID-19) in the UK. Accessed 7th of November 2020 https://coronavirus.data.gov.uk/details/deaths.
-
- Karaglannidis C., Mostert C., Hentschker C. Case characteristics, resource use and outcomes of 10021 patients with COVID-19 admitted to 920 German hospitals: an observational study. Lancet Respir Med. 2020 doi: 10.1016/S2213-2600(20)30316-7. published early online: Published Online July 28, 2020. - DOI - PMC - PubMed
-
- Intensive Care National Audit and Research Centre (2020) ICNARC report on COVID-19 in critical care. 31st of July 2020. Accessed 7th of November: https://www.icnarc.org/Our-Audit/Audits/Cmp/Reports
Grants and funding
LinkOut - more resources
Full Text Sources
