

Audiological results and subjective benefit of an active transcutaneous bone-conduction device in patients with congenital aural atresia
- PMID: 34173875
- PMCID: PMC8986742
- DOI: 10.1007/s00405-021-06938-8
Audiological results and subjective benefit of an active transcutaneous bone-conduction device in patients with congenital aural atresia
Abstract
Purpose: To review functional and subjective benefit after implantation of an active transcutaneous bone conduction device (BCD) in patients with congenital microtia with atresia or stenosis of the external auditory canal.
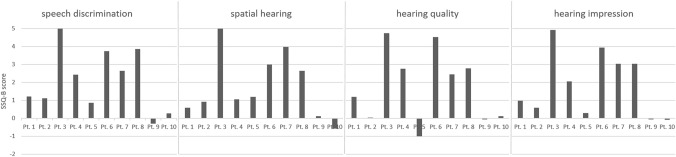
Methods: Retrospective chart analysis and questionnaire on the subjective impression of hearing ( Speech, Spatial and Qualities of Hearing Scale (SSQ-B) of patients treated between 2012 and 2015.
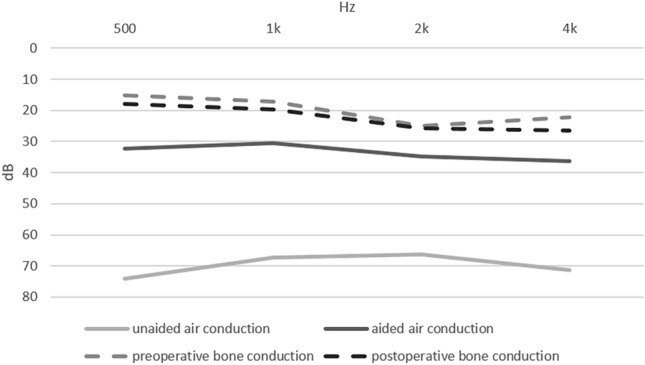
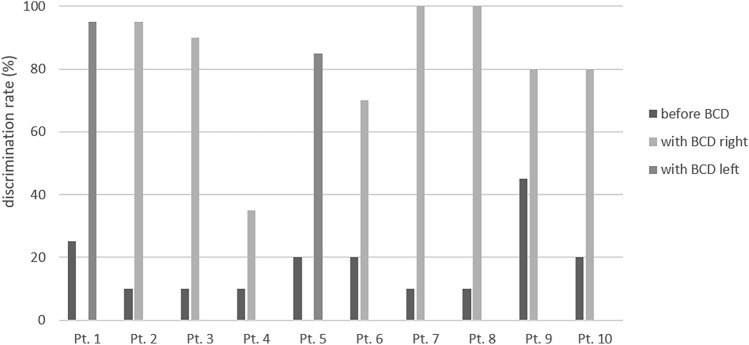
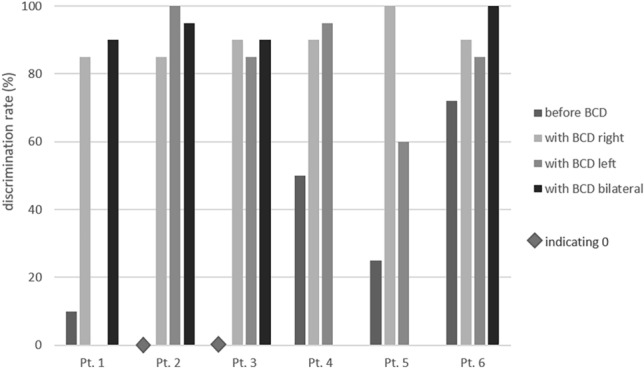
Resultsresults: 18 patients (24 ears) with conductive or mixed hearing loss in unilateral (n = 10) or bilateral (n = 8) atresia were implanted with a BCD. No major complications occurred after implantation. Preoperative unaided air conduction pure tone average at 0.5, 1, 2 and 4 kHz (PTA 4 ) was 69.2 ± 11.7 dB, while postoperative aided PTA 4 was 33.4 ± 6.3 dB, resulting in a mean functional hearing gain of 35.9 +/- 15.6 dB. Preoperatively, the mean monosyllabic word recognition score was 22.9 % ± 22.3 %, which increased to 87.1 % +/- 15.1 % in the aided condition. The Oldenburger Sentence Test at S0N0 revealed a decrease in signal-to-noise-ratio from - 0.58 ± 4.40 dB in the unaided to - 5.67 ± 3.21 dB in the postoperative aided condition for all patients investigated. 15 of 18 patients had a subjective benefit showing a positive SSQ-B score (mean 1.7).
Conclusion: The implantation of an active bone conduction device brings along subjective and functional benefit for patients with conductive or combined hearing loss.
Keywords: Bone conduction device; Bonebridge; Congenital aural atresia; Hearing rehabilitation; SSQ.
© 2021. The Author(s).
Conflict of interest statement
The author have no conflict of interst to declare.
Figures

Similar articles
-
Audiological and subjective outcomes of 100 implanted transcutaneous bone conduction devices and preoperative bone conduction hearing aids in patients with bilateral microtia-atresia.Acta Otolaryngol. 2020 Aug;140(8):675-681. doi: 10.1080/00016489.2020.1762929. Epub 2020 May 20. Acta Otolaryngol. 2020. PMID: 32432498
-
Long-term follow-up of Bonebridge BCI 601 implantation in microtia patients with aural atresia: Acoustic and subjective benefits.J Chin Med Assoc. 2024 Dec 1;87(12):1090-1097. doi: 10.1097/JCMA.0000000000001162. Epub 2024 Sep 10. J Chin Med Assoc. 2024. PMID: 39252162
-
Audiological outcomes in patients with congenital aural atresia implanted with transcutaneous active bone conduction hearing implant.Int J Pediatr Otorhinolaryngol. 2019 Apr;119:54-58. doi: 10.1016/j.ijporl.2019.01.016. Epub 2019 Jan 14. Int J Pediatr Otorhinolaryngol. 2019. PMID: 30665177
-
Multicentric study on surgical information and early safety and performance results with the Bonebridge BCI 602: an active transcutaneous bone conduction hearing implant.Eur Arch Otorhinolaryngol. 2023 Apr;280(4):1565-1579. doi: 10.1007/s00405-022-07792-y. Epub 2023 Jan 10. Eur Arch Otorhinolaryngol. 2023. PMID: 36625869 Free PMC article. Review.
-
Long-term follow-up and review of the Bone Conduction Implant.Hear Res. 2022 Aug;421:108503. doi: 10.1016/j.heares.2022.108503. Epub 2022 Apr 3. Hear Res. 2022. PMID: 35490057 Review.
Cited by
-
Role of early hearing aid experience in speech recognition in patients with bilateral congenital microtia following Bonebridge implantation: a retrospective cohort study.Eur Arch Otorhinolaryngol. 2024 Mar;281(3):1205-1214. doi: 10.1007/s00405-023-08210-7. Epub 2023 Oct 4. Eur Arch Otorhinolaryngol. 2024. PMID: 37792216
-
Long-term safety and subjective satisfaction of Bonebridge and Vibrant Soundbridge in congenital unilateral conductive hearing loss.Acta Otorhinolaryngol Ital. 2024 Oct;44(5):322-332. doi: 10.14639/0392-100X-N2659. Acta Otorhinolaryngol Ital. 2024. PMID: 39526769 Free PMC article.
References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
