

COVID-19 myocarditis: quantitative analysis of the inflammatory infiltrate and a proposed mechanism
- PMID: 34174415
- PMCID: PMC8223028
- DOI: 10.1016/j.carpath.2021.107361
COVID-19 myocarditis: quantitative analysis of the inflammatory infiltrate and a proposed mechanism
Abstract
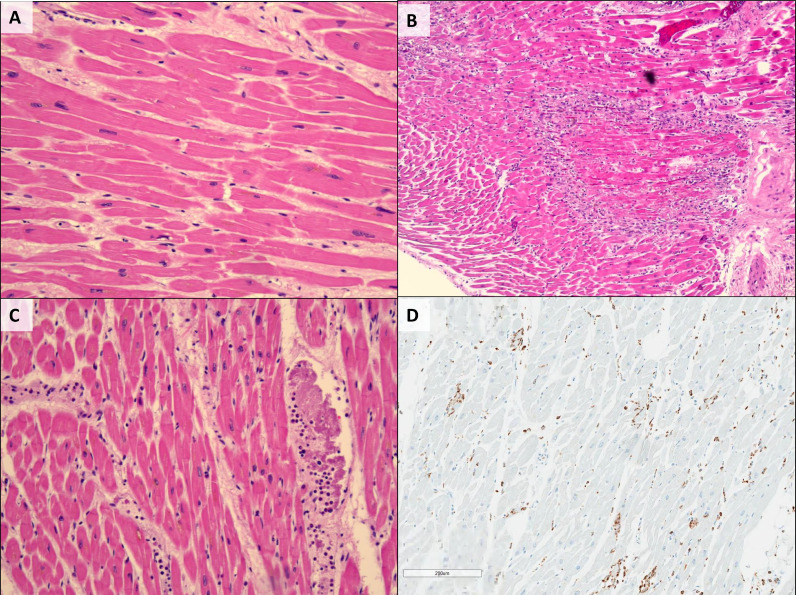
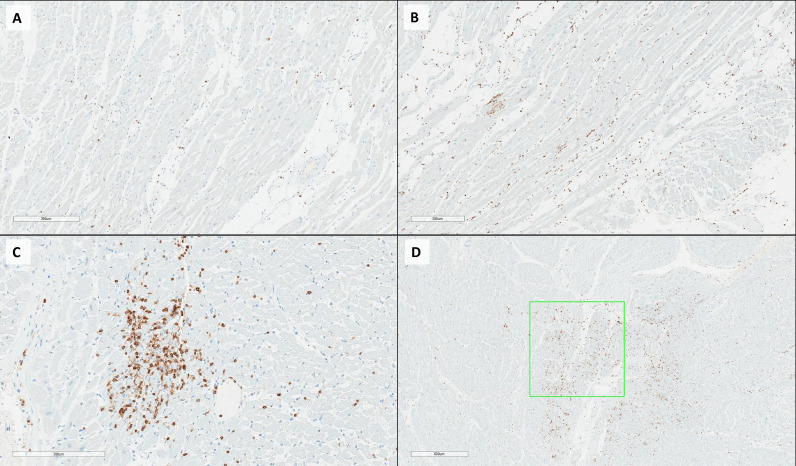
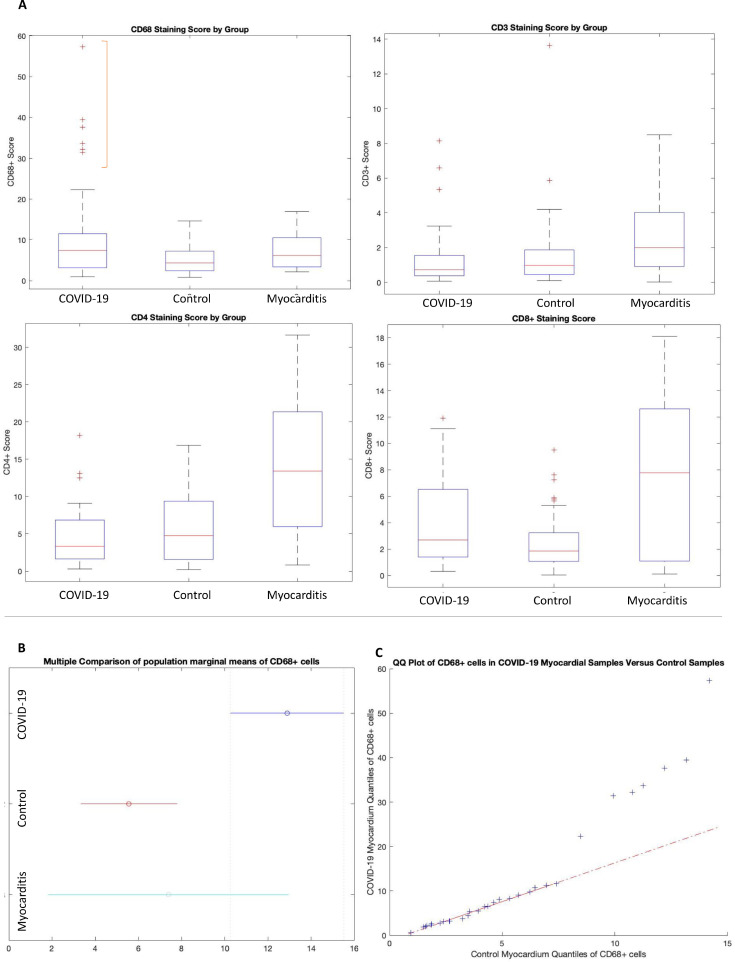
COVID-19 has a significant effect upon the cardiovascular system. While a number of different cardiovascular histopathologies have been described at post-mortem examination, the incidence of typical viral myocarditis in COVID-19 positive patients appears very low [1-3]. In this study, we further characterize and quantify the inflammatory cell infiltrate in a COVID-19 study cohort and compare the findings to both an age and disease matched control cohort and a cohort of patients diagnosed with typical inflammatory myocarditis. All study and control cohorts had 1 or more of the comorbidities most commonly associated with severe disease (hypertension, type II diabetes, obesity, or known cardiovascular disease). The results demonstrate a skewed distribution of the number of CD68+ cells in COVID-19 hearts, with upper quantiles showing a significant increase as compared to both matched control hearts, and those with myocarditis. In contrast, hearts from typical inflammatory myocarditis contained increased numbers of CD4+, and CD8+ cells compared to both COVID-19 and control cohorts. In conclusion, the presence of an increased number of CD68+ cells suggests that COVID-19 may incite a form of myocarditis different from typical viral myocarditis, and associated with diffusely infiltrative cells of monocytes/macrophage lineage.
Keywords: CD68 cells; COVID-19; SARS-CoV-2; autopsy, myocarditis, heart, inflammation, macrophages.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
References
-
- Fox SE, Li G, Akmatbekov A, Harbert JL, Lameira FS, Brown JQ, et al. Unexpected features of cardiac pathology in COVID-19 infection. Circulation. 2020;142:1123–1125. - PubMed
-
- Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020;581:465–469. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
