

Long-term results after mitral valve surgery using minimally invasive versus sternotomy approach: a propensity matched comparison of a large single-center series
- PMID: 34174818
- PMCID: PMC8236182
- DOI: 10.1186/s12872-021-02121-3
Long-term results after mitral valve surgery using minimally invasive versus sternotomy approach: a propensity matched comparison of a large single-center series
Abstract
Background: Mitral valve (MV) surgery has traditionally been performed by conventional sternotomy (CS), but more recently minimally invasive surgery (MIS) has become another treatment option. The aim of this study is to compare short- and long-term results of MV surgery after CS and MIS.
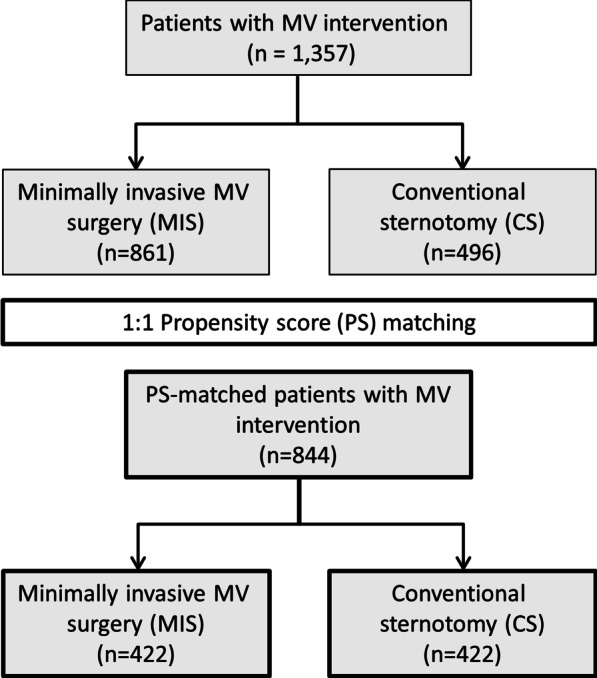
Methods: This study was a retrospective propensity-matched analysis of MV operations between January 2005 and December 2015.
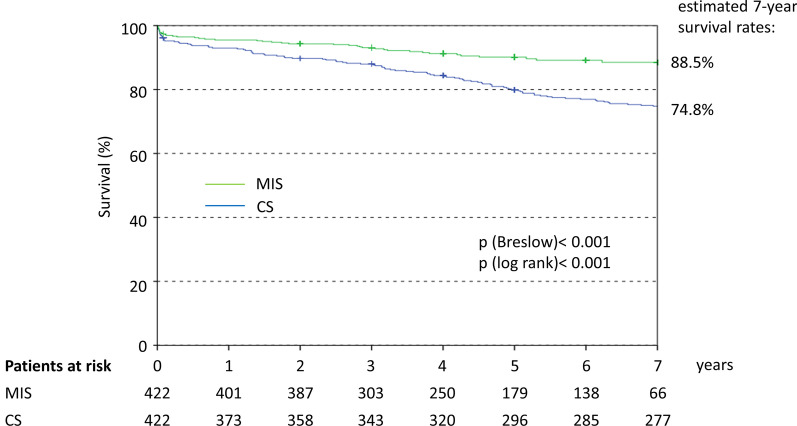
Results: Among 1357 patients, 496 underwent CS and 861 MIS. Matching resulted in 422 patients per group. The procedure time was longer with MIS than CS (192 vs. 185 min; p = 0.002) as was cardiopulmonary bypass time (133 vs. 101 min; p < 0.001) and X-clamp time (80 vs. 71 min; p < 0.001). 'Short-term' successful valve repair was higher with MIS (96.0% vs. 76.0%, p < 0.001). Length of hospital stay was shorter in MIS than CS patients (10 vs. 11 days; p = 0.001). There was no difference in the overall 30-day mortality rate. Cardiovascular death was lower after MIS (1.2%) compared with CS (3.8%; OR 0.30; 95%CI 0.11-0.84). The difference did not remain significant after adjustment for procedural differences (aOR 0.40; 95%CI 0.13-1.25). Pacemaker was required less often after MIS (3.3%) than CS (11.2%; aOR 0.31; 95%CI 0.16-0.61), and acute renal failure was less common (2.1% vs. 11.9%; aOR 0.22; 95%CI 0.10-0.48). There were no significant differences with respect to rates of stroke, myocardial infarction or repeat MV surgery. The 7-year survival rate was significantly better after MIS (88.5%) than CS (74.8%; aHR 0.44, 95%CI 0.31-0.64).
Conclusion: This study demonstrates that good results for MV surgery can be obtained with MIS, achieving a high MV repair rate, low peri-procedural morbidity and mortality, and improved long-term survival.
Keywords: Minimally invasive mitral valve surgery; Mitral valve; Mitral valve repair; Outcomes; Sternotomy.
Conflict of interest statement
Peter Bramlage received research funding from Edwards Lifesciences related and unrelated to the present work. The other authors have no conflict of interest to disclose.
Figures
Similar articles
-
Minithoracotomy versus sternotomy in mitral valve surgery: meta-analysis from recent matched and randomized studies.J Cardiothorac Surg. 2023 Apr 6;18(1):101. doi: 10.1186/s13019-023-02229-x. J Cardiothorac Surg. 2023. PMID: 37024952 Free PMC article. Review.
-
Minimally invasive mitral valve surgery in a non-high volume center.Scand Cardiovasc J. 2025 Dec;59(1):2514743. doi: 10.1080/14017431.2025.2514743. Epub 2025 Jun 13. Scand Cardiovasc J. 2025. PMID: 40464524
-
Does full sternotomy have more significant impact than the cardiopulmonary bypass time in patients of mitral valve surgery?J Cardiothorac Surg. 2018 Apr 14;13(1):29. doi: 10.1186/s13019-018-0719-4. J Cardiothorac Surg. 2018. PMID: 29653554 Free PMC article.
-
Propensity-Matched Comparison of Two Different Access Modes for Minimally Invasive Mitral Valve Surgery.Semin Thorac Cardiovasc Surg. 2020 Spring;32(1):36-44. doi: 10.1053/j.semtcvs.2019.08.008. Epub 2019 Aug 21. Semin Thorac Cardiovasc Surg. 2020. PMID: 31445088
-
Right minithoracotomy versus median sternotomy for reoperative mitral valve surgery: a systematic review and meta-analysis of observational studies.Eur J Cardiothorac Surg. 2018 Nov 1;54(5):817-825. doi: 10.1093/ejcts/ezy173. Eur J Cardiothorac Surg. 2018. PMID: 29688301
Cited by
-
Minimally Invasive Mitral Valve Replacement in a Patient With a Giant Left Atrium.Cureus. 2025 Jun 5;17(6):e85423. doi: 10.7759/cureus.85423. eCollection 2025 Jun. Cureus. 2025. PMID: 40630349 Free PMC article.
-
An Individualized, Less-Invasive Surgical Approach Algorithm Improves Outcome in Elderly Patients Undergoing Mitral Valve Surgery.J Cardiovasc Dev Dis. 2023 Jan 11;10(1):28. doi: 10.3390/jcdd10010028. J Cardiovasc Dev Dis. 2023. PMID: 36661923 Free PMC article.
-
Safety and Efficacy of the Transaxillary Access for Minimally Invasive Mitral Valve Surgery-A Propensity Matched Competitive Analysis.Medicina (Kaunas). 2022 Dec 15;58(12):1850. doi: 10.3390/medicina58121850. Medicina (Kaunas). 2022. PMID: 36557053 Free PMC article.
-
Minithoracotomy versus sternotomy in mitral valve surgery: meta-analysis from recent matched and randomized studies.J Cardiothorac Surg. 2023 Apr 6;18(1):101. doi: 10.1186/s13019-023-02229-x. J Cardiothorac Surg. 2023. PMID: 37024952 Free PMC article. Review.
-
An international survey-based assessment of minimally invasive mitral valve surgery.Interdiscip Cardiovasc Thorac Surg. 2023 Oct 4;37(4):ivad154. doi: 10.1093/icvts/ivad154. Interdiscip Cardiovasc Thorac Surg. 2023. PMID: 37713462 Free PMC article.
References
-
- Al Otaibi A, Gupta S, Belley-Cote EP, Alsagheir A, Spence J, Parry D, et al. Mini-thoracotomy vs. cnventional sternotomy mitral valve surgery: a systematic review and meta-analysis. J Cardiovasc Surg (Torino) 2017;58(3):489–96. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
