

Sex differences in the associations between adiposity distribution and cardiometabolic risk factors in overweight or obese individuals: a cross-sectional study
- PMID: 34174845
- PMCID: PMC8234731
- DOI: 10.1186/s12889-021-11316-4
Sex differences in the associations between adiposity distribution and cardiometabolic risk factors in overweight or obese individuals: a cross-sectional study
Abstract
Background: We aimed to assess the associations between adiposity distribution and cardiometabolic risk factors among overweight and obese adults in China, and to demonstrate the sex differences in these associations.
Methods: A total of 1221 participants (455 males and 766 females) were included in this study. Percentage of body fat (PBF) of the whole body and regional areas, including arm, thigh, trunk, android, and gynoid, were measured by the dual-energy X-ray absorptiometry method. Central adiposity was measured by waist circumference. Clustered cardiometabolic risk was defined as the presence of two or more of the six cardiometabolic risk factors, namely, high triglyceride, low high density lipoprotein, elevated glucose, elevated blood pressure, elevated high sensitivity C-reactive protein, and low adiponectin. Linear regression models and multivariate logistic regression models were used to assess the associations between whole body or regional PBF and cardiometabolic risk factors.
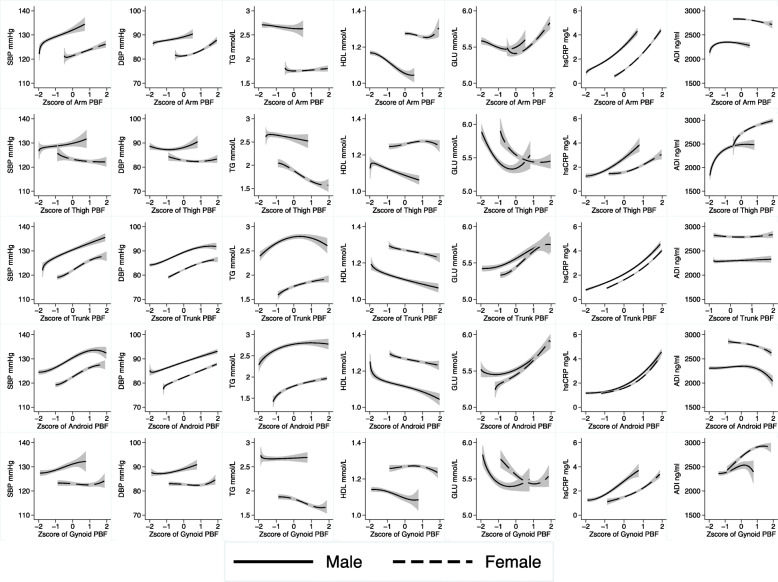
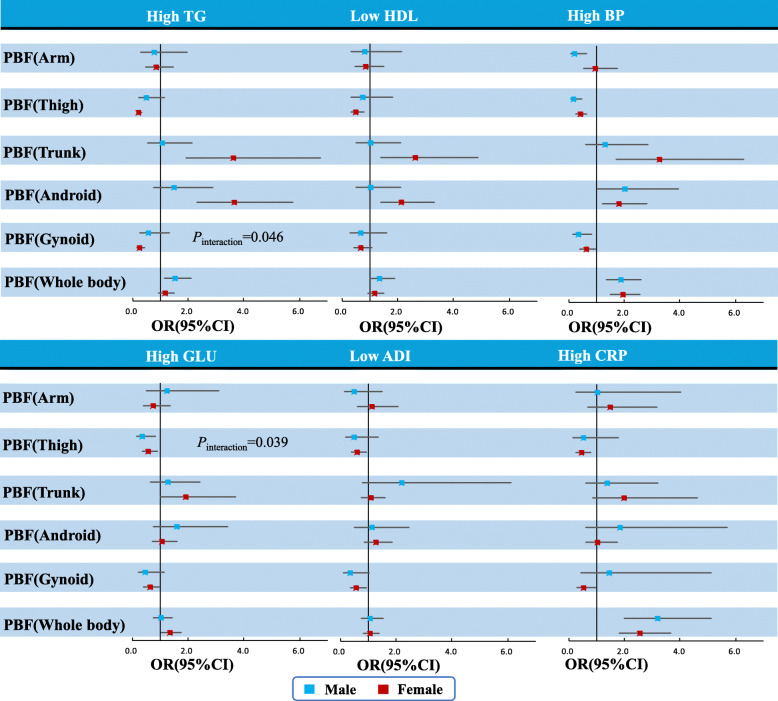
Results: In females, except arm adiposity, other regional fat (thigh, trunk, android, gynoid) and whole-body PBF are significantly associated with clustered cardiometabolic risk, adjusting for age, smoking, alcohol drinking, physical activity, and whole-body PBF. One-SD increase in Z scores of the thigh and gynoid PBF were significantly associated with 80 and 78% lower odds of clustered cardiometabolic risk (OR: 0.20, 95%CI: 0.12-0.35 and OR: 0.22, 95%CI: 0.12-0.41). Trunk, android and whole-body PBF were significantly associated with higher odds of clustered risk with OR of 1.90 (95%CI:1.02-3.55), 2.91 (95%CI: 1.75-4.85), and 2.01 (95%CI: 1.47-2.76), respectively. While in males, one-SD increase in the thigh and gynoid PBF are associated with 94% (OR: 0.06, 95%CI: 0.02-0.23) and 83% lower odds (OR: 0.17, 95%CI: 0.05-0.57) of clustered cardiometabolic risk, respectively. Android and whole-body PBF were associated with higher odds of clustered cardiometabolic risk (OR: 3.39, 95%CI: 1.42-8.09 and OR: 2.45, 95%CI: 1.53-3.92), but the association for trunk PBF was not statistically significant (OR: 1.16, 95%CI: 0.42-3.19).
Conclusions: Adiposity distribution plays an important role in the clustered cardiometabolic risk in participants with overweight and obese and sex differences were observed in these associations. In general, central obesity (measured by android PBF) could be the best anthropometric measurement for screening people at risk for CVD risk factors for both men and women. Upper body fat tends to be more detrimental to cardiometabolic health in women than in men, whereas lower body fat is relatively more protective in men than in women.
Keywords: Cardiometabolic health; Fat distribution; Overweight and obesity; Sex difference.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Association of regional body fat with metabolic risks in Chinese women.Public Health Nutr. 2014 Oct;17(10):2316-24. doi: 10.1017/S1368980013002668. Epub 2013 Oct 22. Public Health Nutr. 2014. PMID: 24148901 Free PMC article.
-
[Association between regional fat mass and risk of nonalcoholic fatty liver disease in overweight/obese adults].Wei Sheng Yan Jiu. 2022 Sep;51(5):753-760. doi: 10.19813/j.cnki.weishengyanjiu.2022.05.013. Wei Sheng Yan Jiu. 2022. PMID: 36222034 Chinese.
-
DXA-Derived vs Standard Anthropometric Measures for Predicting Cardiometabolic Risk in Middle-Aged Australian Men and Women.J Clin Densitom. 2022 Jul-Sep;25(3):299-307. doi: 10.1016/j.jocd.2022.01.006. Epub 2022 Jan 10. J Clin Densitom. 2022. PMID: 35177350
-
Whole-Fat or Reduced-Fat Dairy Product Intake, Adiposity, and Cardiometabolic Health in Children: A Systematic Review.Adv Nutr. 2020 Jul 1;11(4):928-950. doi: 10.1093/advances/nmaa011. Adv Nutr. 2020. PMID: 32119732 Free PMC article.
-
Overweight, Obesity, and CVD Risk: a Focus on Visceral/Ectopic Fat.Curr Atheroscler Rep. 2022 Apr;24(4):185-195. doi: 10.1007/s11883-022-00996-x. Epub 2022 Mar 2. Curr Atheroscler Rep. 2022. PMID: 35235165 Review.
Cited by
-
Comparison of bioelectrical body and visceral fat indices and anthropometric measures in relation to type 2 diabetes by sex among Chinese adults, a cross-sectional study.Front Public Health. 2023 Nov 7;11:1001397. doi: 10.3389/fpubh.2023.1001397. eCollection 2023. Front Public Health. 2023. PMID: 38026280 Free PMC article.
-
Mediating Roles of hsCRP, TNF-α and Adiponectin on the Associations between Body Fat and Fatty Liver Disease among Overweight and Obese Adults.Biology (Basel). 2021 Sep 10;10(9):895. doi: 10.3390/biology10090895. Biology (Basel). 2021. PMID: 34571772 Free PMC article.
-
Regional adipose distribution and metabolically unhealthy phenotype in Chinese adults: evidence from China National Health Survey.Environ Health Prev Med. 2025;30:5. doi: 10.1265/ehpm.24-00154. Environ Health Prev Med. 2025. PMID: 39828368 Free PMC article.
-
Sexual Dimorphism in Cardiovascular Biomarkers: Clinical and Research Implications.Circ Res. 2022 Feb 18;130(4):578-592. doi: 10.1161/CIRCRESAHA.121.319916. Epub 2022 Feb 17. Circ Res. 2022. PMID: 35175850 Free PMC article. Review.
-
Risk Factors and Cellular Differences in Heart Failure: The Key Role of Sex Hormones.Biomedicines. 2023 Nov 14;11(11):3052. doi: 10.3390/biomedicines11113052. Biomedicines. 2023. PMID: 38002052 Free PMC article. Review.
References
-
- Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019; 92(6–10. doi: 10.1016/j.metabol.2018.09.005. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
