

Long-term effectiveness of elderly health care voucher scheme strategies: a system dynamics simulation analysis
- PMID: 34174858
- PMCID: PMC8236172
- DOI: 10.1186/s12889-021-11280-z
Long-term effectiveness of elderly health care voucher scheme strategies: a system dynamics simulation analysis
Abstract
Background: The elderly healthcare voucher (EHCV) scheme is expected to lead to an increase in the number of elderly people selecting private primary healthcare services and reduce reliance on the public sector in Hong Kong. However, studies thus far have reported that this scheme has not received satisfactory responses. In this study, we examined changes in the ratio of visits between public and private doctors in primary care (to measure reliance on the public sector) for different strategic scenarios in the EHCV scheme.
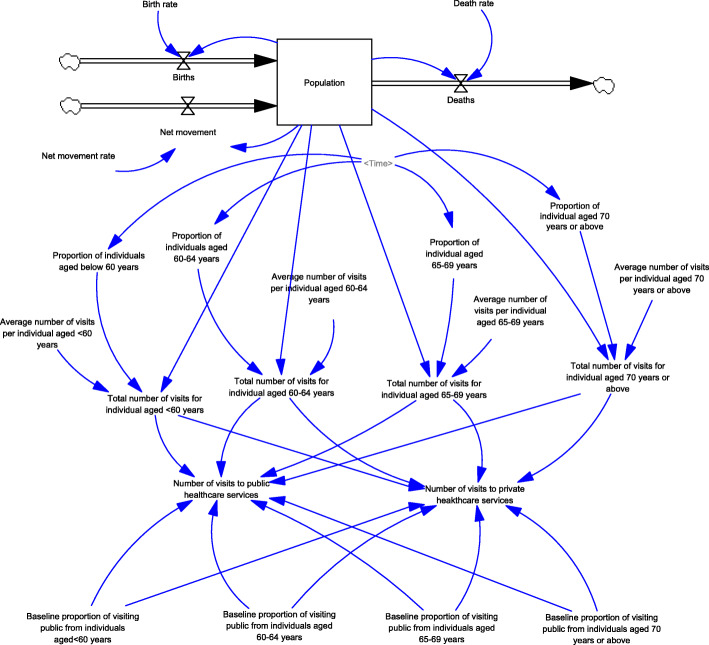
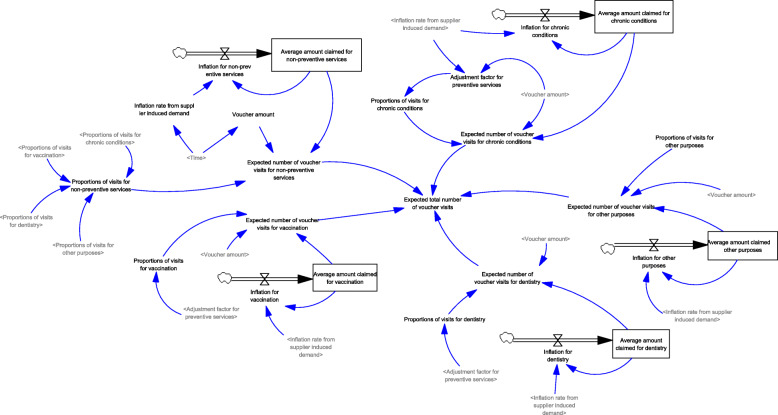
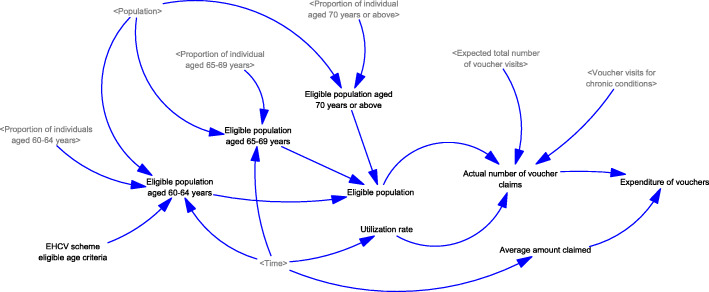
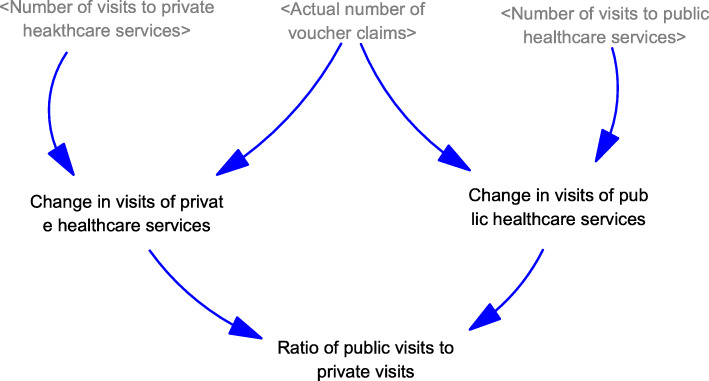
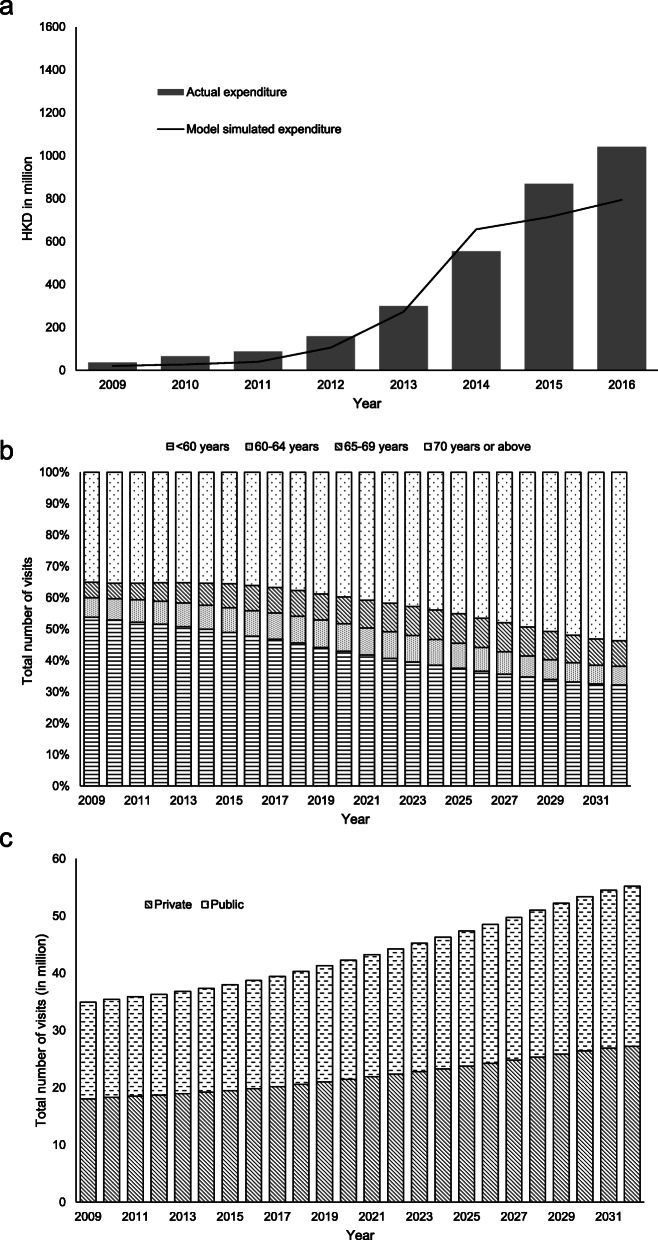
Methods: Based on comments from an expert panel, a system dynamics model was formulated to simulate the impact of various enhanced strategies in the scheme: increasing voucher amounts, lowering the age eligibility, and designating vouchers for chronic conditions follow-up. Data and statistics for the model calibration were collected from various sources.
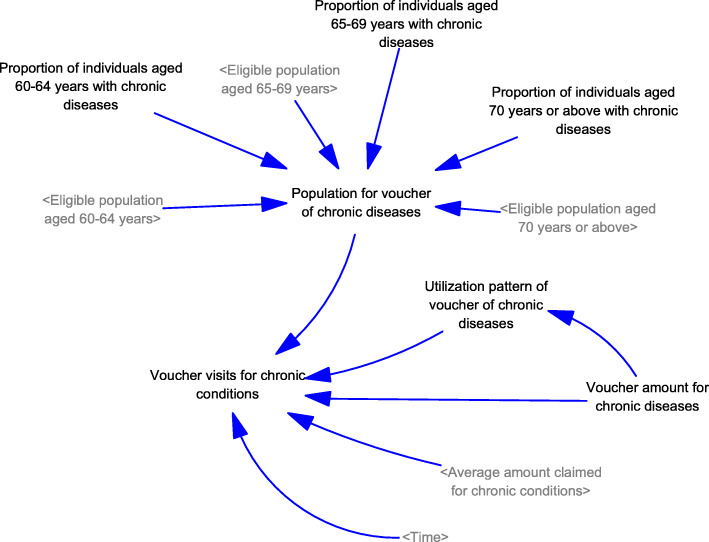
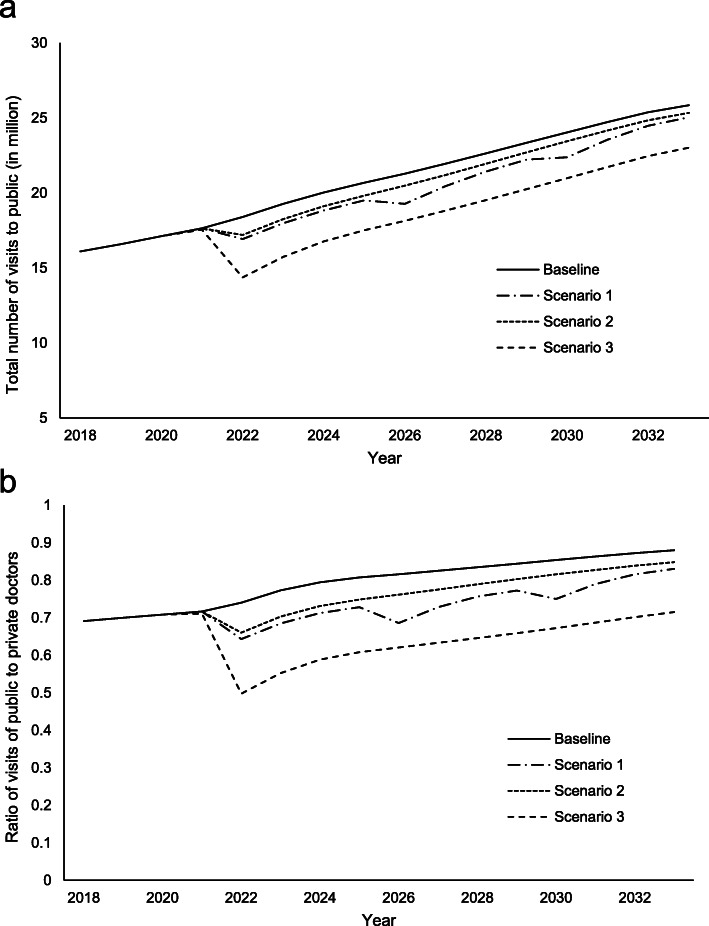
Results: The simulation results show that the current EHCV scheme is unable to reduce the utilization of public healthcare services, as well as the ratio of visits between public and private primary care among the local aging population. When comparing three different tested scenarios, even if the increase in the annual voucher amount could be maintained at the current pace or the age eligibility can be lowered to include those aged 60 years, the impact on shifts from public-to-private utilization were insignificant. The public-to-private ratio could only be marginally reduced from 0.74 to 0.64 in the first several years. Nevertheless, introducing a chronic disease-oriented voucher could result in a significant drop of 0.50 in the public-to-private ratio during the early implementation phase. However, the effect could not be maintained for an extended period.
Conclusions: Our findings will assist officials in improving the design of the EHCV scheme, within the wider context of promoting primary care among the elderly. We suggest that an additional chronic disease-oriented voucher can serve as an alternative strategy. The scheme must be redesigned to address more specific objectives or provide a separate voucher that promotes under-utilized healthcare services (e.g., preventive care), instead of services designed for unspecified reasons, which may lead to concerns regarding exploitation.
Keywords: Chronic; Elderly care; Elderly healthcare voucher; Financial incentive; Simulation; System dynamics.
Conflict of interest statement
As a member of the editorial board of the journal, KCC was not involved in the peer review process of this article. The other authors declare that they have no competing interests.
Figures
Similar articles
-
Can vouchers make a difference to the use of private primary care services by older people? Experience from the healthcare reform programme in Hong Kong.BMC Health Serv Res. 2011 Oct 7;11:255. doi: 10.1186/1472-6963-11-255. BMC Health Serv Res. 2011. PMID: 21978140 Free PMC article.
-
What is the long term impact of voucher scheme on primary care? Findings from a repeated cross sectional study using propensity score matching.BMC Health Serv Res. 2019 Nov 21;19(1):875. doi: 10.1186/s12913-019-4707-8. BMC Health Serv Res. 2019. PMID: 31752826 Free PMC article.
-
Healthcare vouchers for better elderly services? Input from private healthcare service providers in Hong Kong.Health Soc Care Community. 2022 Feb;30(2):e357-e369. doi: 10.1111/hsc.13203. Epub 2020 Oct 31. Health Soc Care Community. 2022. PMID: 33128419
-
Synergies between veterinarians and para-professionals in the public and private sectors: organisational and institutional relationships that facilitate the process of privatising animal health services in developing countries.Rev Sci Tech. 2004 Apr;23(1):115-35; discussion 391-401. doi: 10.20506/rst.23.1.1472. Rev Sci Tech. 2004. PMID: 15200091 Review.
-
Effectively engaging the private sector through vouchers and contracting - A case for analysing health governance and context.Soc Sci Med. 2015 Nov;145:193-200. doi: 10.1016/j.socscimed.2015.05.021. Epub 2015 May 14. Soc Sci Med. 2015. PMID: 26004065 Review.
Cited by
-
Feasibility of a telephone-delivered educational intervention for knowledge transfer of COVID-19-related information to older adults in Hong Kong: a pre-post-pilot study.Pilot Feasibility Stud. 2022 Oct 6;8(1):228. doi: 10.1186/s40814-022-01169-y. Pilot Feasibility Stud. 2022. PMID: 36203186 Free PMC article.
-
Equality and social determinants of spatial accessibility, availability, and affordability to primary health care in Hong Kong, a descriptive study from the perspective of spatial analysis.BMC Health Serv Res. 2022 Nov 17;22(1):1364. doi: 10.1186/s12913-022-08760-2. BMC Health Serv Res. 2022. PMID: 36397059 Free PMC article.
-
Supervision for the Public Health Services for Older Adults Under the Background of Government Purchasing: An Evolutionary Game Analysis Framework.Front Public Health. 2022 May 16;10:881330. doi: 10.3389/fpubh.2022.881330. eCollection 2022. Front Public Health. 2022. PMID: 35651859 Free PMC article.
References
-
- Census and Statistics Department. Hong Kong Population Projections 2015–2064. [http://www.censtatd.gov.hk/hkstat/sub/sp190.jsp?productCode=B1120015] 2015.
-
- Food and Health Bureau, HKSAR Government. Factsheet on Healthcare Reform. http://www.fhb.gov.hk/beStrong/files/consultation/factsheettext_eng.pdf Accessed: 2015.
-
- Census and Statistics Department . Thematic Household Survey Report No.40. 2009. p. 43.
-
- Food and Health Bureau, HKSAR . My Health My Choice. Healthcare Reform Second Stage Consultation. Hong Kong: Consultation Document; 2010.
-
- Background of Elderly Health Care Voucher Scheme. The Government of HKSAR. http://www.hcv.gov.hk/eng/pub_background.htm 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
