

Hybrid emergency rooms reduce the requirement of blood transfusion in patients with severe trauma
- PMID: 34174929
- PMCID: PMC8236173
- DOI: 10.1186/s13017-021-00377-w
Hybrid emergency rooms reduce the requirement of blood transfusion in patients with severe trauma
Abstract
Background: A hybrid emergency room (ER) is defined as an emergency unit with four functions-performing resuscitation, computed tomography (CT), surgery, and angiography. However, the safety and efficacy of performing CT in a hybrid ER are unclear in primary surveys. Therefore, this study aimed to evaluate the safety and clinical effects of hybrid ERs.
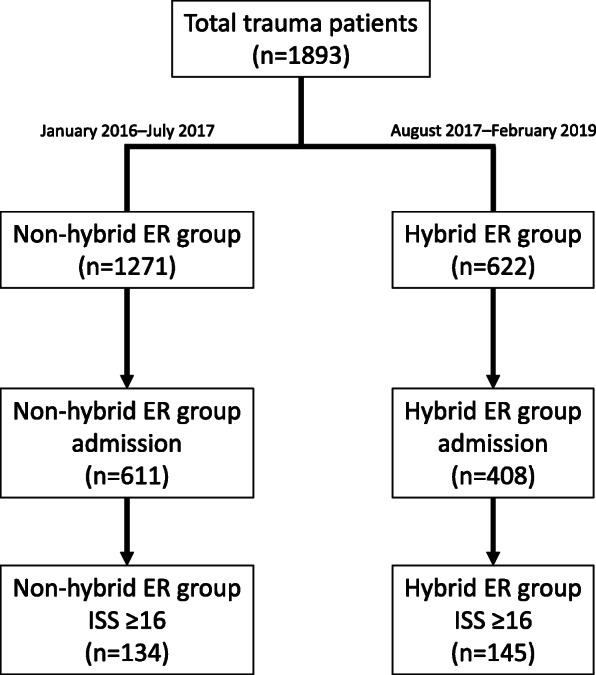
Methods: This retrospective observational study used data from the Shimane University Hospital Trauma Database from January 2016 to February 2019. Hospitalized patients with severe trauma and an injury severity score of ≥ 16 were divided into the non-hybrid ER group (n = 134) and the hybrid ER group (n = 145). The time from arrival to CT and interventions and the number of in-hospital survivors, preventable trauma deaths (PTD), and unexpected survivors (US) were assessed in both groups. Further, the amount of blood transfused was compared between the groups using propensity score matching.
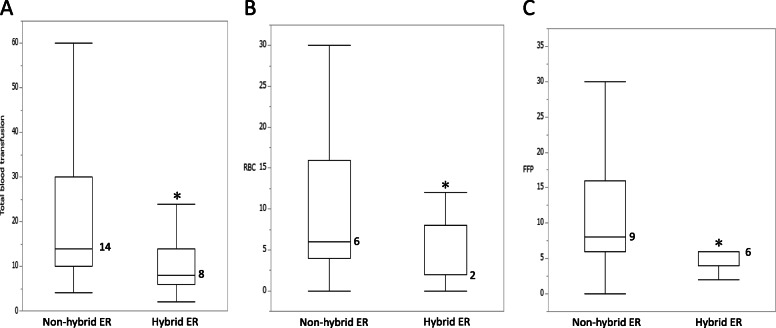
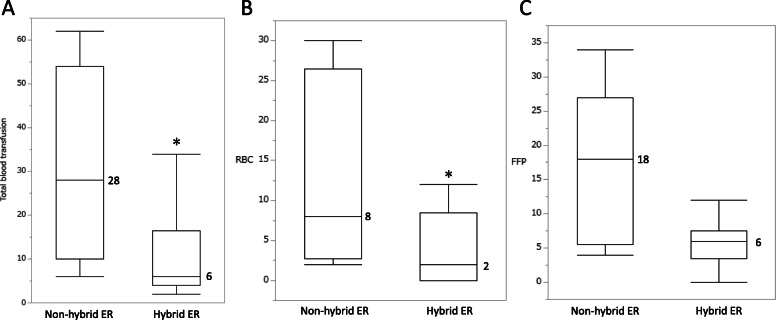
Results: The time from arrival to CT and interventions was significantly reduced in the hybrid ER group compared to that in the non-hybrid ER group (25 vs. 6 min; p < 0.0001 and 101 vs. 41 min; p = 0.0007, respectively). There was no significant difference in the rate of in-hospital survivors (96.9% vs. 96.3%; p = 0.770), PTD (0% vs. 0%), and US (9.0 vs. 6.2%; p = 0.497) between the groups. The amount of blood transfused was significantly lower in the hybrid ER group than in the non-hybrid ER group (whole blood 14 vs. 8, p = 0.004; red blood cell 6 vs. 2, p = 0.012; fresh frozen plasma 9 vs. 6, p = 0.021). This difference was maintained after propensity score matching (whole blood 28 [10-54] vs. 6 [4-16.5], p = 0.015; RBC 8 [2.75-26.5] vs. 2 [0-8.5], p = 0.020, 18 [5.5-27] vs. 6 [3.5-7.5], p = 0.057).
Conclusions: The study results suggest that trauma treatment in a hybrid ER is as safe as conventional treatment performed in a non-hybrid ER. Further, hybrid ERs, which can reduce the time for trauma surveys and treatment, do not require patient transfer and can reduce the amount of blood transfused during resuscitation.
Keywords: Blood transfusion; Hemostasis; Hybrid emergency room.
Conflict of interest statement
Hiroaki Watanabe received lecture fees and travel expenses from Canon Medical Systems for educational lectures in Japan. The rest of the authors declare that they have no competing interests.
Figures

Similar articles
-
The Survival Benefit of a Novel Trauma Workflow that Includes Immediate Whole-body Computed Tomography, Surgery, and Interventional Radiology, All in One Trauma Resuscitation Room: A Retrospective Historical Control Study.Ann Surg. 2019 Feb;269(2):370-376. doi: 10.1097/SLA.0000000000002527. Ann Surg. 2019. PMID: 28953551 Free PMC article.
-
Hybrid emergency room shows maximum effect on trauma resuscitation when used in patients with higher severity.J Trauma Acute Care Surg. 2021 Feb 1;90(2):232-239. doi: 10.1097/TA.0000000000003020. J Trauma Acute Care Surg. 2021. PMID: 33165282
-
The association between timing of CT and outcomes for severe trauma patients: analysis of a nationwide trauma registry.Eur J Trauma Emerg Surg. 2025 Mar 26;51(1):150. doi: 10.1007/s00068-025-02839-1. Eur J Trauma Emerg Surg. 2025. PMID: 40140101
-
First establishment of a new table-rotated-type hybrid emergency room system.Scand J Trauma Resusc Emerg Med. 2018 Sep 17;26(1):80. doi: 10.1186/s13049-018-0532-z. Scand J Trauma Resusc Emerg Med. 2018. PMID: 30223859 Free PMC article. Review.
-
[Hemoglobin-oriented and coagulation factor-based algorithm : Effect on transfusion needs and standardized mortality rate in massively transfused trauma patients].Anaesthesist. 2015 Nov;64(11):828-38. doi: 10.1007/s00101-015-0093-8. Epub 2015 Oct 9. Anaesthesist. 2015. PMID: 26453580 Review. German.
Cited by
-
Treatment strategy for severe trauma patients requiring aortic occlusion for impending cardiopulmonary arrest in the hybrid emergency room.Acute Med Surg. 2024 Jan 29;11(1):e928. doi: 10.1002/ams2.928. eCollection 2024 Jan-Dec. Acute Med Surg. 2024. PMID: 38293705 Free PMC article.
-
A systematic review of emergency room laparotomy in patients with severe abdominal trauma.Sci Rep. 2025 Jan 22;15(1):2808. doi: 10.1038/s41598-025-87241-y. Sci Rep. 2025. PMID: 39843466 Free PMC article.
-
Hybrid emergency room: Installation, establishment, and innovation in the emergency department.Acute Med Surg. 2023 May 31;10(1):e856. doi: 10.1002/ams2.856. eCollection 2023 Jan-Dec. Acute Med Surg. 2023. PMID: 37266185 Free PMC article. Review.
-
Correlation between the Injury Site and Trauma Mechanism in Severely Injured Patients with Blunt Trauma.Emerg Med Int. 2022 May 24;2022:8372012. doi: 10.1155/2022/8372012. eCollection 2022. Emerg Med Int. 2022. PMID: 37020739 Free PMC article.
-
Timing and volume of transfusion for adult major trauma patients with hemorrhagic shock: a registry-based cohort study.Trauma Surg Acute Care Open. 2024 Feb 7;9(1):e001248. doi: 10.1136/tsaco-2023-001248. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38347897 Free PMC article.
References
-
- Sierink JC, Treskes K, Edwards MJ, Beuker BJ, den Hartog D, Hohmann J, et al. Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial. Lancet. 2016;388(10045):673–683. doi: 10.1016/S0140-6736(16)30932-1. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
