

Breast cancer risk factors in relation to molecular subtypes in breast cancer patients from Kenya
- PMID: 34174935
- PMCID: PMC8235821
- DOI: 10.1186/s13058-021-01446-3
Breast cancer risk factors in relation to molecular subtypes in breast cancer patients from Kenya
Abstract
Background: Few studies have investigated risk factor heterogeneity by molecular subtypes in indigenous African populations where prevalence of traditional breast cancer (BC) risk factors, genetic background, and environmental exposures show marked differences compared to European ancestry populations.
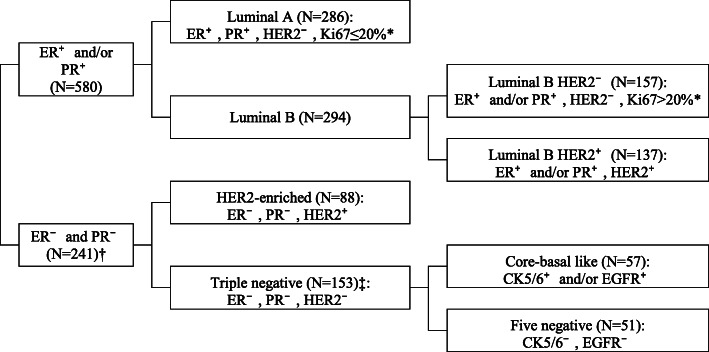
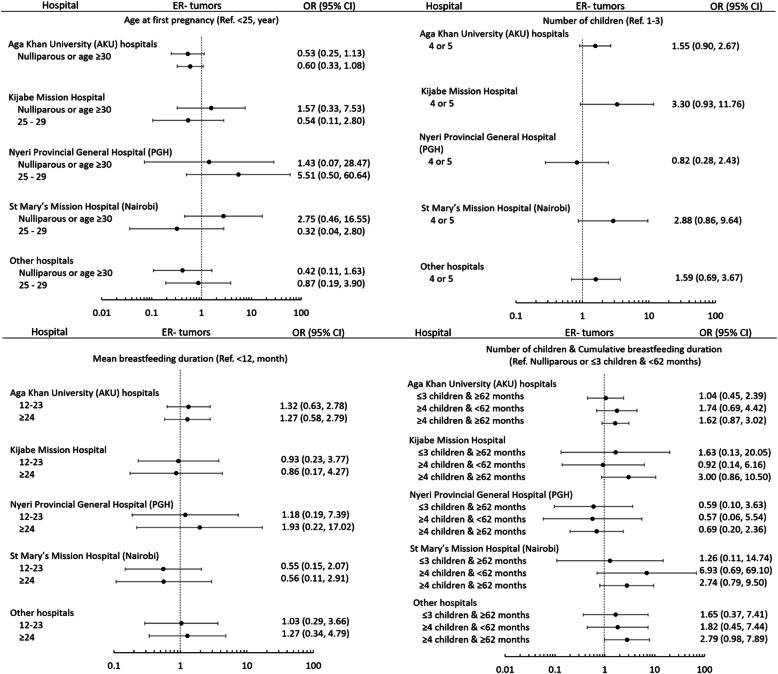
Methods: We conducted a case-only analysis of 838 pathologically confirmed BC cases recruited from 5 groups of public, faith-based, and private institutions across Kenya between March 2012 to May 2015. Centralized pathology review and immunohistochemistry (IHC) for key markers (ER, PR, HER2, EGFR, CK5-6, and Ki67) was performed to define subtypes. Risk factor data was collected at time of diagnosis through a questionnaire. Multivariable polytomous logistic regression models were used to determine associations between BC risk factors and tumor molecular subtypes, adjusted for clinical characteristics and risk factors.
Results: The median age at menarche and first pregnancy were 14 and 21 years, median number of children was 3, and breastfeeding duration was 62 months per child. Distribution of molecular subtypes for luminal A, luminal B, HER2-enriched, and triple negative (TN) breast cancers was 34.8%, 35.8%, 10.7%, and 18.6%, respectively. After adjusting for covariates, compared to patients with ER-positive tumors, ER-negative patients were more likely to have higher parity (OR = 2.03, 95% CI = (1.11, 3.72), p = 0.021, comparing ≥ 5 to ≤ 2 children). Compared to patients with luminal A tumors, luminal B patients were more likely to have lower parity (OR = 0.45, 95% CI = 0.23, 0.87, p = 0.018, comparing ≥ 5 to ≤ 2 children); HER2-enriched patients were less likely to be obese (OR = 0.36, 95% CI = 0.16, 0.81, p = 0.013) or older age at menopause (OR = 0.38, 95% CI = 0.15, 0.997, p = 0.049). Body mass index (BMI), either overall or by menopausal status, did not vary significantly by ER status. Overall, cumulative or average breastfeeding duration did not vary significantly across subtypes.
Conclusions: In Kenya, we found associations between parity-related risk factors and ER status consistent with observations in European ancestry populations, but differing associations with BMI and breastfeeding. Inclusion of diverse populations in cancer etiology studies is needed to develop population and subtype-specific risk prediction/prevention strategies.
Keywords: Breast cancer; Kenya; Molecular subtypes; Risk factors; Sub-Saharan Africa.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Joko-Fru WY, Miranda-Filho A, Soerjomataram I, Egue M, Akele-Akpo MT, N’da G, et al. Breast cancer survival in sub-Saharan Africa by age, stage at diagnosis and human development index: A population-based registry study. Int J Cancer. 2020;146(5):1208–1218. doi: 10.1002/ijc.32406. - DOI - PMC - PubMed
-
- McCormack V, McKenzie F, Foerster M, Zietsman A, Galukande M, Adisa C, et al. Breast cancer survival and survival gap apportionment in sub-Saharan Africa (ABC-DO): a prospective cohort study. Lancet Glob Heal [Internet]. 2020 1 [cited 2021 Jan 9];8(9):e1203–12. Available from: www.thelancet.com/lancetgh - PMC - PubMed
-
- Sayed S, Moloo Z, Ngugi A, Allidina A, Ndumia R, Mutuiri A, et al. Breast camps for awareness and early diagnosis of breast cancer in countries with limited resources: A multidisciplinary model from Kenya. Oncologist [Internet]. 2016;21(9):1138–1148. doi: 10.1634/theoncologist.2016-0004. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
