

Serological abnormalities that predict progression to systemic autoimmune rheumatic diseases in antinuclear antibody-positive individuals
- PMID: 34175923
- PMCID: PMC8889298
- DOI: 10.1093/rheumatology/keab501
Serological abnormalities that predict progression to systemic autoimmune rheumatic diseases in antinuclear antibody-positive individuals
Abstract
Objective: We investigated the autoantibody (autoAb) profiles in ANA+ individuals lacking systemic autoimmune rheumatic disease (SARD) and early SARD patients to determine the key differences between these groups and identify factors that are associated with an increased risk of symptomatic progression within the next 2 years in ANA+ individuals.
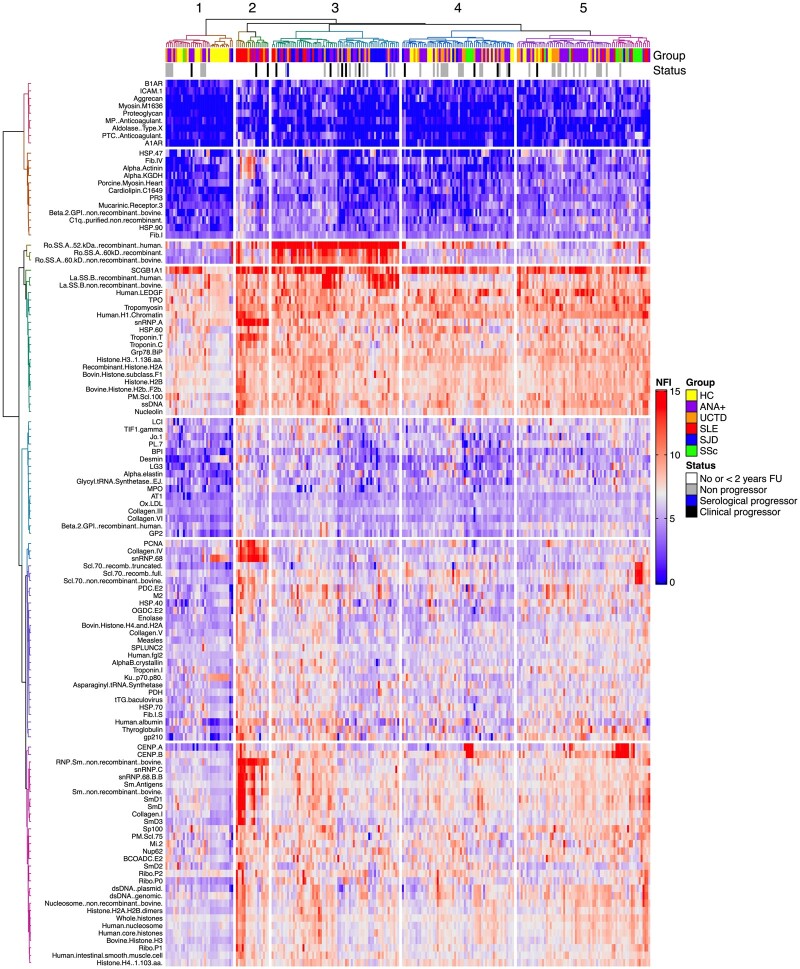
Methods: Using custom antigen (Ag) microarrays, 144 IgM and IgG autoAbs were surveyed in 84 asymptomatic and 123 symptomatic (48 UCTD and 75 SARD patients) ANA+ individuals. AutoAbs were compared in ANA+ individuals lacking a SARD diagnosis with ≥2 years follow-up (n = 52), including all those who demonstrated progression (n = 14) during this period, with changes over time assessed in a representative subset.
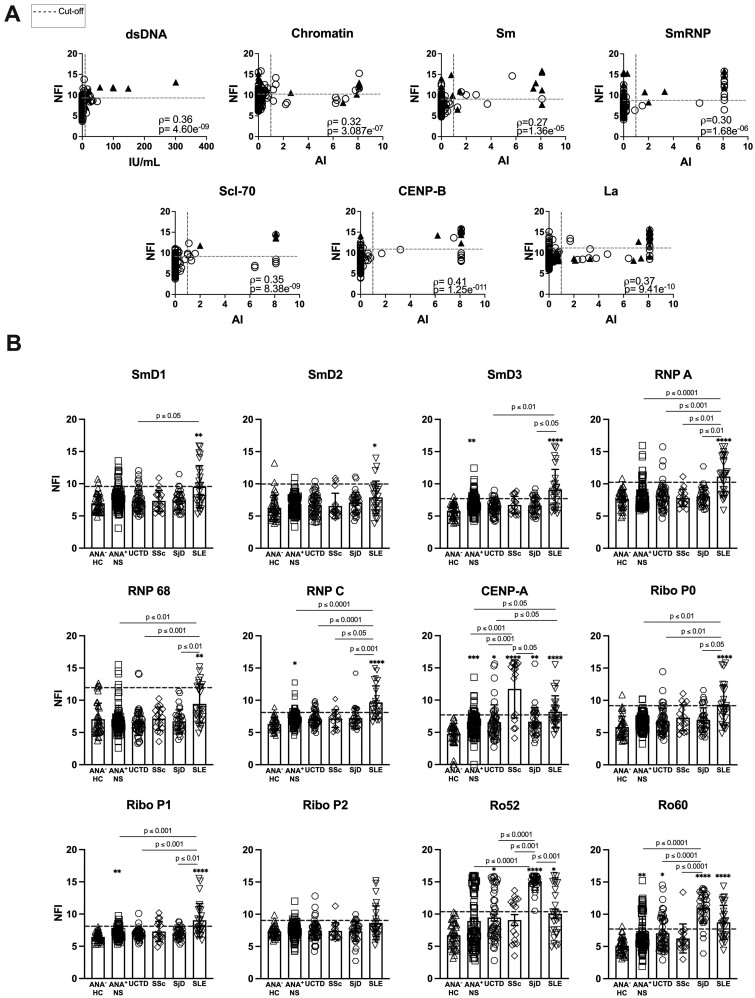
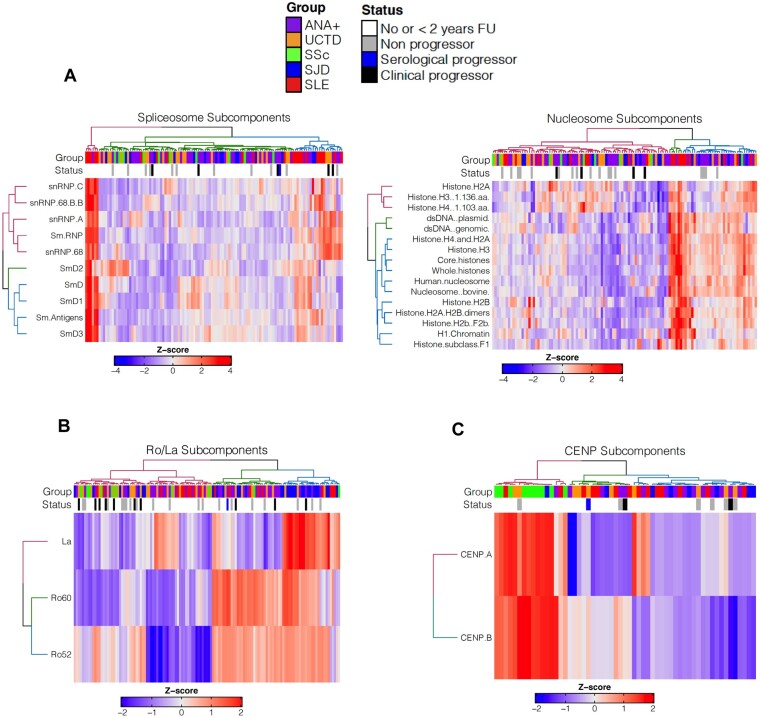
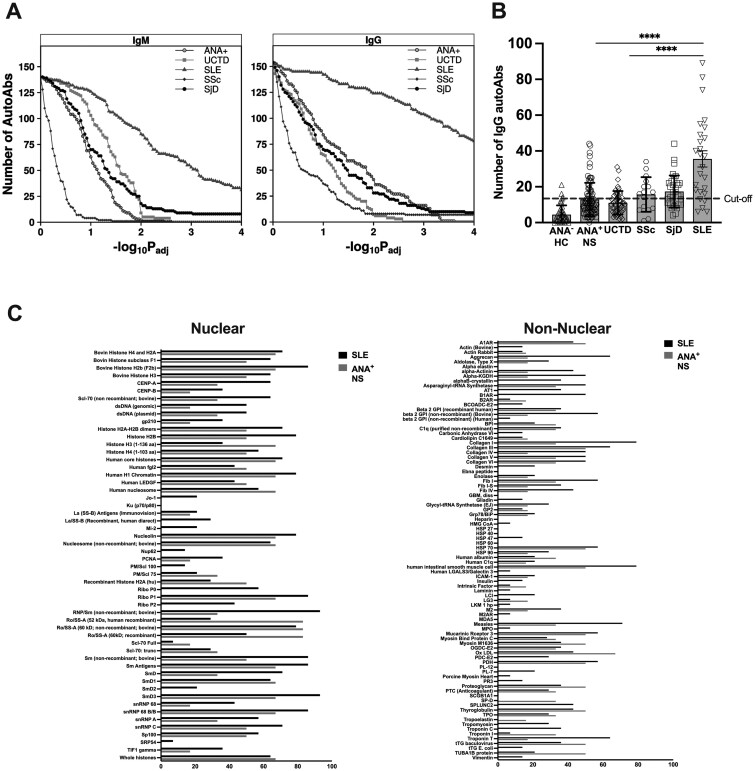
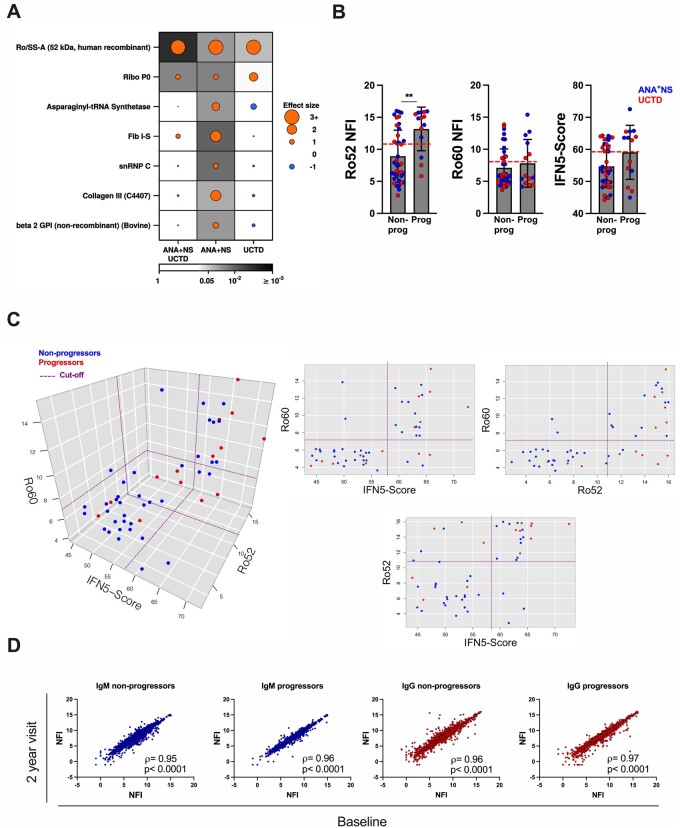
Results: We show that ANA+ individuals have autoAb to many self-Ags that are not being captured by current screening techniques and very high levels of these autoAbs are predominantly restricted to early SARD patients, with SLE patients displaying reactivity to many more autoAgs than the other groups. In general, the symptoms that developed in progressors mirrored those seen in SARD patients with similar patterns of autoAbs. Only anti-Ro52 Abs were found to predict progression (positive predictive value 46%, negative predictive value 89%). Surprisingly, over 2 years of follow-up the levels of autoAbs remained remarkably stable regardless of whether individuals progressed or not.
Conclusion: Our findings strongly argue that development of assays with an expanded set of auto-Ags and enhanced dynamic range would improve the diagnostic and prognostic ability of autoAb testing.
Keywords: Ro52 antigen; SLE; antinuclear antibodies; microarray analysis; rheumatic diseases.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- McClain MT, Arbuckle MR, Heinlen LD. et al. The prevalence, onset, and clinical significance of antiphospholipid antibodies prior to diagnosis of systemic lupus erythematosus. Arthritis Rheum 2004;50:1226–32. - PubMed
