

Longitudinal prediction of hospital-acquired acute kidney injury in COVID-19: a two-center study
- PMID: 34176087
- PMCID: PMC8235913
- DOI: 10.1007/s15010-021-01646-1
Longitudinal prediction of hospital-acquired acute kidney injury in COVID-19: a two-center study
Abstract
Background: To investigate the temporal characteristics of clinical variables of hospital-acquired acute kidney injury (AKI) in COVID-19 patients and to longitudinally predict AKI onset.
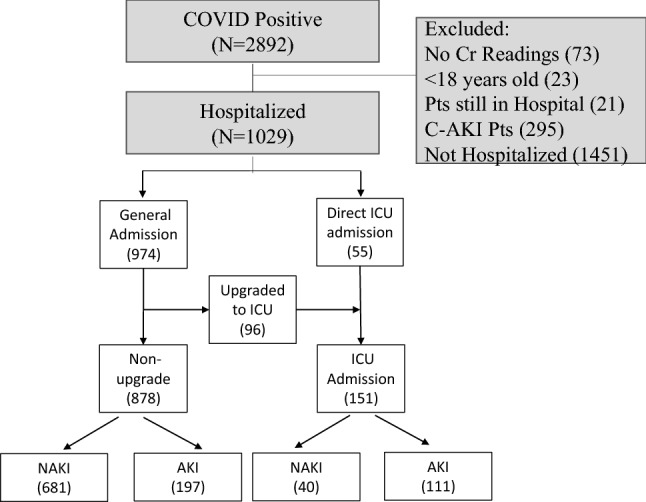
Methods: There were 308 hospital-acquired AKI and 721 non-AKI (NAKI) COVID-19 patients from Stony Brook Hospital (New York, USA) data, and 72 hospital-acquired AKI and 303 NAKI COVID-19 patients from Tongji Hospital (Wuhan, China). Demographic, comorbidities, and longitudinal (3 days before and 3 days after AKI onset) clinical variables were used to compute odds ratios for and longitudinally predict hospital-acquired AKI onset.
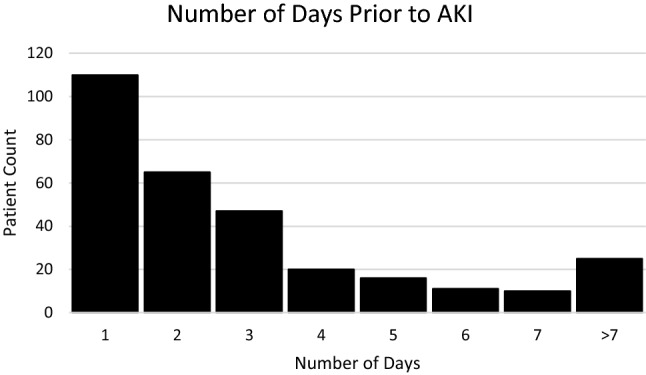
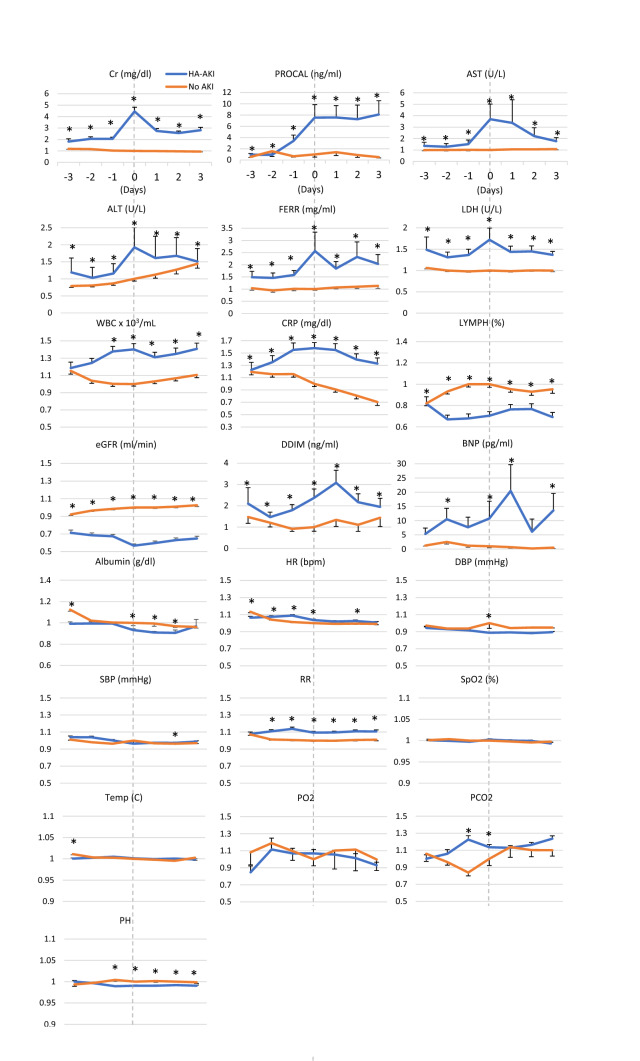
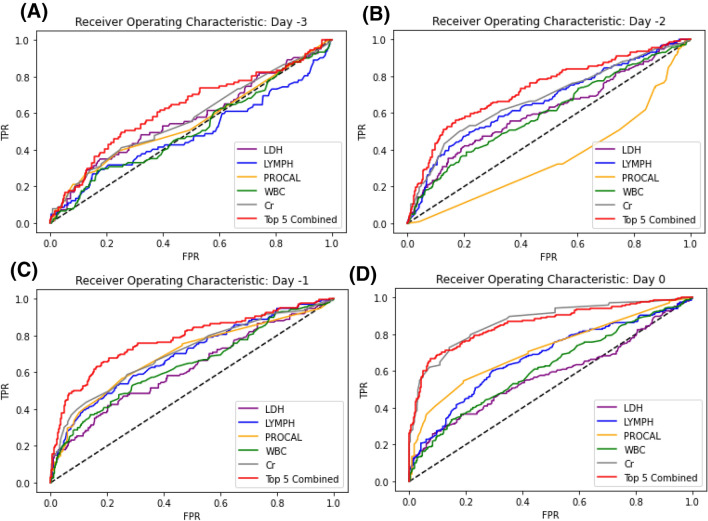
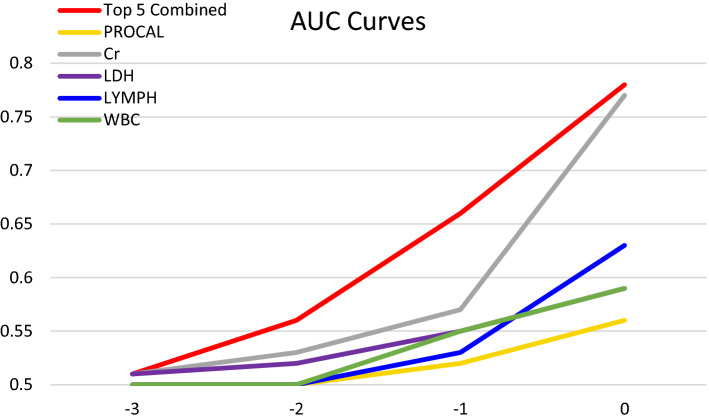
Results: COVID-19 patients with AKI were more likely to die than NAKI patients (31.5% vs 6.9%, adjusted p < 0.001, OR = 4.67 [95% CI 3.1, 7.0], Stony Brook data). AKI developed on average 3.3 days after hospitalization. Procalcitonin was elevated prior to AKI onset (p < 0.05), peaked, and remained elevated (p < 0.05). Alanine aminotransferase, aspartate transaminase, ferritin, and lactate dehydrogenase peaked the same time as creatinine, whereas D-dimer and brain natriuretic peptide peaked a day later. C-reactive protein, white blood cell and lymphocyte showed group differences - 2 days prior (p < 0.05). Top predictors were creatinine, procalcitonin, white blood cells, lactate dehydrogenase, and lymphocytes. They predicted AKI onset with areas under curves (AUCs) of 0.78, 0.66, and 0.56 at 0, - 1, and - 2 days prior, respectively. When tested on the Tongji Hospital data, the AUCs were 0.80, 0.79, and 0.77, respectively.
Conclusions: Time-locked longitudinal data provide insight into AKI progression. Commonly clinical variables reasonably predict AKI onset a few days prior. This work may lead to earlier recognition of AKI and treatment to improve clinical outcomes.
Keywords: AKI; Chronic kidney disease; Cytokine storm; D-Dimer; Lactate dehydrogenase; Multiorgan failure; Predictive model; SARS-CoV-2.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
Authors declare no conflicts of interest.
Figures

Similar articles
-
Long-short-term memory machine learning of longitudinal clinical data accurately predicts acute kidney injury onset in COVID-19: a two-center study.Int J Infect Dis. 2022 Sep;122:802-810. doi: 10.1016/j.ijid.2022.07.034. Epub 2022 Jul 22. Int J Infect Dis. 2022. PMID: 35872094 Free PMC article.
-
Longitudinal progression of clinical variables associated with graded liver injury in COVID-19 patients.Hepatol Int. 2021 Aug;15(4):1018-1026. doi: 10.1007/s12072-021-10228-0. Epub 2021 Jul 15. Hepatol Int. 2021. PMID: 34268650 Free PMC article.
-
[Acute kidney injury in patients hospitalized with COVID-19 in Wuhan, China: a single-center retrospective observational study].Nan Fang Yi Ke Da Xue Xue Bao. 2021 Feb 25;41(2):157-163. doi: 10.12122/j.issn.1673-4254.2021.02.01. Nan Fang Yi Ke Da Xue Xue Bao. 2021. PMID: 33624587 Free PMC article.
-
[Clinical characteristics and risk factors of acute kidney injury in coronavirus disease 2019].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Apr;32(4):407-411. doi: 10.3760/cma.j.cn121430-20200302-00198. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32527342 Chinese.
-
Acute kidney injury in COVID-19: are kidneys the target or just collateral damage? A comprehensive assessment of viral RNA and AKI rate in patients with COVID-19.Curr Opin Urol. 2021 Jul 1;31(4):363-368. doi: 10.1097/MOU.0000000000000901. Curr Opin Urol. 2021. PMID: 33989230 Free PMC article. Review.
Cited by
-
COVID-19 Patients in the COVID-19 Recovery and Engagement (CORE) Clinics in the Bronx.Diagnostics (Basel). 2022 Dec 30;13(1):119. doi: 10.3390/diagnostics13010119. Diagnostics (Basel). 2022. PMID: 36611411 Free PMC article.
-
Renal Manifestations and their Association with Mortality and Length of Stay in COVID-19 Patients at a Safety-net Hospital.J Crit Care Med (Targu Mures). 2022 May 12;8(2):80-88. doi: 10.2478/jccm-2022-0010. eCollection 2022 Apr. J Crit Care Med (Targu Mures). 2022. PMID: 35950159 Free PMC article.
-
Long-term outcomes of hospitalized patients with SARS-CoV-2/COVID-19 with and without neurological involvement: 3-year follow-up assessment.PLoS Med. 2024 Apr 4;21(4):e1004263. doi: 10.1371/journal.pmed.1004263. eCollection 2024 Apr. PLoS Med. 2024. PMID: 38573873 Free PMC article.
-
Characteristics of COVID-19 patients with multiorgan injury across the pandemic in a large academic health system in the Bronx, New York.Heliyon. 2023 Apr;9(4):e15277. doi: 10.1016/j.heliyon.2023.e15277. Epub 2023 Apr 6. Heliyon. 2023. PMID: 37051049 Free PMC article.
-
Incidence, characteristics, and risk factors of new liver disorders 3.5 years post COVID-19 pandemic in the Montefiore Health System in Bronx.PLoS One. 2024 Jun 13;19(6):e0303151. doi: 10.1371/journal.pone.0303151. eCollection 2024. PLoS One. 2024. PMID: 38870207 Free PMC article.
References
-
- Oliveira CB, Lima CAD, Vajgel G, Campos Coelho AV, Sandrin-Garcia P. High burden of acute kidney injury in COVID-19 pandemic: systematic review and meta-analysis. J Clin Pathol. 2020;7:89. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
