

Multifocal Pyoderma Gangrenosum with an Underlying Hemophagocytic Lymphohistiocytosis: Case Report and the Review of the Literature
- PMID: 34176093
- PMCID: PMC8322207
- DOI: 10.1007/s13555-021-00571-3
Multifocal Pyoderma Gangrenosum with an Underlying Hemophagocytic Lymphohistiocytosis: Case Report and the Review of the Literature
Abstract
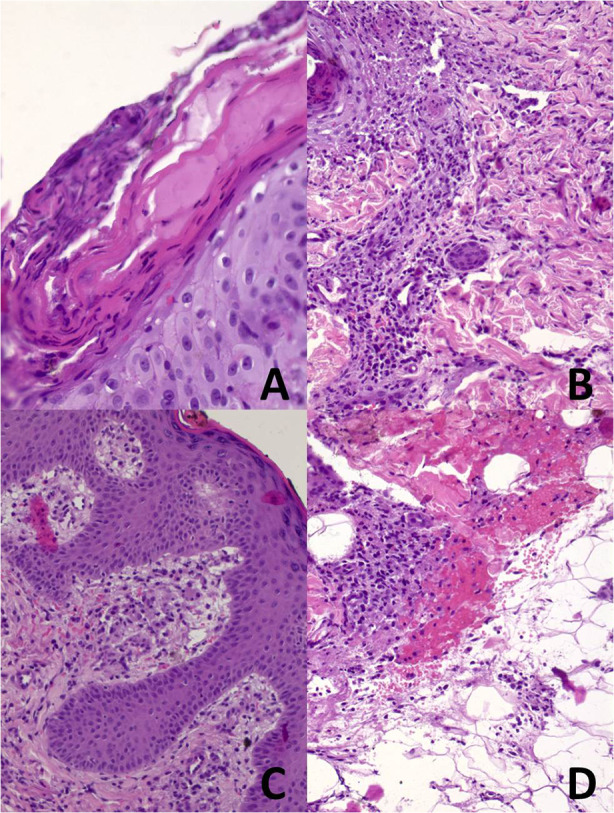
Pyoderma gangrenosum (PG) is an uncommon, serious, ulcerating skin disease of uncertain etiology. It manifests as a noninfectious, progressive necrosis of the skin characterized by sterile neutrophilic infiltrates. It seems to be a disorder of the immune system. PG is associated with certain underlying conditions in at least 50% of cases. Therefore, it is important to look carefully for comorbidities in every patient with PG and treat them adequately to improve the prognosis. Here, we demonstrate a 35-year-old man diagnosed with multifocal PG and hemophagocytic lymphohistiocytosis (HLH) with fatal outcome, despite combined, long-term, intensive dermatological and hematological treatment with high doses of steroids, cyclosporin, intravenous immunoglobulins (IVIG), HLH-2004 protocol with intravenously administered etoposide, and anakinra. This case is presented owing to the extremely rare coexistence of PG and HLH and the related diagnostic and therapeutic difficulties. It is also worth underlying that the diagnosis of HLH should perhaps be considered in the presence of a high percentage of double-negative T lymphocytes (DNTs) in flow cytometry, after excluding the diagnosis of lymphoma and leukemia. In this article we have also performed and present the critical literature review of local and systemic options in the management of PG lesions based on a detailed search of the PubMed database.
Keywords: Anakinra; DNTs; Double-negative T lymphocytes; Etoposide; HLH; Hemophagocytic lymphohistiocytosis; Pyoderma gangrenosum.
© 2021. The Author(s).
Figures





Similar articles
-
Generalized Pyoderma Gangrenosum Associated with Ulcerative Colitis: Successful Treatment with Infliximab and Azathioprine.Acta Dermatovenerol Croat. 2016 Apr;24(1):83-5. Acta Dermatovenerol Croat. 2016. PMID: 27149138
-
Adult-onset Primary Hemophagocytic Lymphohistiocytosis: Reporting a Rare Case with Review of Literature.Cureus. 2020 Jan 21;12(1):e6723. doi: 10.7759/cureus.6723. Cureus. 2020. PMID: 32133251 Free PMC article.
-
Hemophagocytic lymphohistiocytosis during treatment of intracranial multifocal germinoma: a case report and literature review.Front Oncol. 2024 Mar 12;14:1264926. doi: 10.3389/fonc.2024.1264926. eCollection 2024. Front Oncol. 2024. PMID: 38532931 Free PMC article.
-
Histoplasmosis-Associated Hemophagocytic Lymphohistiocytosis: A Review of the Literature.Can J Infect Dis Med Microbiol. 2019 Oct 1;2019:7107326. doi: 10.1155/2019/7107326. eCollection 2019. Can J Infect Dis Med Microbiol. 2019. PMID: 31662810 Free PMC article. Review.
-
Etoposide combined with ruxolitinib for refractory hemophagocytic lymphohistiocytosis during pregnancy: a case report and literature review.Hematology. 2019 Dec;24(1):751-756. doi: 10.1080/16078454.2020.1838708. Hematology. 2019. PMID: 33138732 Review.
Cited by
-
Disrupted Redox Regulation and Inflammatory Response in Pyoderma Gangrenosum.Life (Basel). 2025 Apr 6;15(4):611. doi: 10.3390/life15040611. Life (Basel). 2025. PMID: 40283167 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
