

Bruns' nystagmus revisited: A sign of stroke in patients with the acute vestibular syndrome
- PMID: 34176187
- PMCID: PMC8456911
- DOI: 10.1111/ene.14997
Bruns' nystagmus revisited: A sign of stroke in patients with the acute vestibular syndrome
Abstract
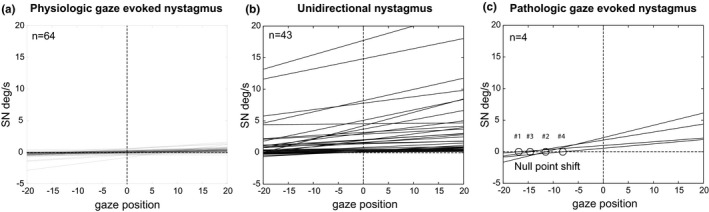
Objective: Gaze-evoked nystagmus (GEN) is a central sign in patients with the acute vestibular syndrome (AVS); however, discriminating between a pathological and a physiologic GEN is a challenge. Here we evaluate GEN in patients with AVS.
Methods: In this prospective cross-sectional study, we used video-oculography (VOG) to compare GEN in the light (target at 15° eccentric) in 64 healthy subjects with 47 patients seen in the emergency department (ED) who had AVS; 35 with vestibular neuritis and 12 with stroke. All patients with an initial non-diagnostic MRI received a confirmatory, delayed MRI as a reference standard in detecting stroke.
Results: Healthy subjects with GEN had a time constant of centripetal drift >18 s. VOG identified pathologic GEN (time constant ≤ 18 s) in 33% of patients with vestibular strokes, specificity was 100%, accuracy was 83%. Results were equivalent to examination by a clinical expert. As expected, since all patients with GEN had a SN in straight-ahead position, they showed the pattern of a Bruns' nystagmus.
Conclusions: One third of patients with AVS due to central vestibular strokes had a spontaneous SN in straight-ahead gaze and a pathological GEN, producing the pattern of a Bruns' nystagmus with a shift of the null position. The localization of the side of the lesion based on the null was not consistent, presumably because the circuits underlying gaze-holding are widespread in the brainstem and cerebellum. Nevertheless, automated quantification of GEN with VOG was specific, and accurately identified patients in the ED with AVS due to strokes.
Keywords: Bruns’ nystagmus; HINTS; acute vestibular syndrome; gaze-evoked nystagmus; gaze-holding nystagmus.
© 2021 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
None of the investigators has any relevant financial interests, activities, relationships, or affiliations that represent a relevant financial conflict of interest with respect to the conduct or analysis of this study. TCS holds an endowed professorship sponsored by Touring Club Switzerland. The sponsor has no influence on the direction and content of the research conducted.
Figures




References
-
- Leigh RJ, Zee DS. The Neurology of Eye Movements. Oxford, UK: Oxford University Press; 2015.
-
- Kim HA, Yi HA, Lee H. Failure of fixation suppression of spontaneous nystagmus in cerebellar infarction: frequency, pattern, and a possible structure. Cerebellum. 2016;15:182‐189. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
