

Remission of Angiographically Confirmed Minocycline-induced Renal Polyarteritis Nodosa: A Case Report and Literature Review
- PMID: 34176836
- PMCID: PMC8810245
- DOI: 10.2169/internalmedicine.7340-21
Remission of Angiographically Confirmed Minocycline-induced Renal Polyarteritis Nodosa: A Case Report and Literature Review
Abstract
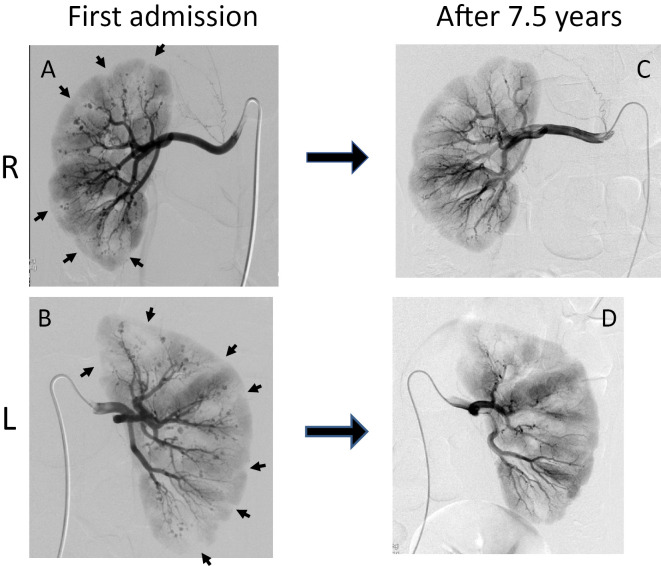
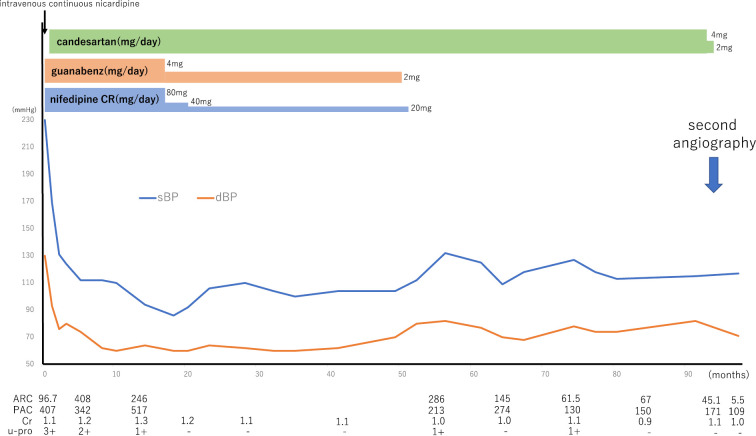
A 23-year-old man presented with severe hypertension. Based on his history of minocycline treatment for over three years and clinical symptoms, such as myalgias and renovascular hypertension with multiple intrarenal aneurysms, he was diagnosed with minocycline-induced renal polyarteritis nodosa (PAN). After minocycline treatment cessation and management of the hypertension, his blood pressure, renin-aldosterone levels, and urinary protein levels gradually improved. Seven and a half years later, repeated angiography found that the aneurysms had resolved. This is the first report in English describing a case of minocycline-induced renal PAN that was reversed functionally and morphologically without steroids or immunosuppressive drugs.
Keywords: aneurysms; angiography; drug-induced vasculitis; minocycline; polyarteritis nodosa; renovascular hypertension.
Conflict of interest statement
Figures


Similar articles
-
Minocycline-induced renal polyarteritis nodosa.BMJ Case Rep. 2012 Aug 13;2012:bcr2012006503. doi: 10.1136/bcr-2012-006503. BMJ Case Rep. 2012. PMID: 22891025 Free PMC article.
-
Polyarteritis nodosa-like vasculitis in association with minocycline use: a single-center case series.Semin Arthritis Rheum. 2012 Oct;42(2):213-21. doi: 10.1016/j.semarthrit.2012.03.006. Epub 2012 Jun 15. Semin Arthritis Rheum. 2012. PMID: 22704357
-
Minocycline-induced cutaneous polyarteritis nodosa.J Clin Rheumatol. 2007 Jun;13(3):146-9. doi: 10.1097/RHU.0b013e3180690693. J Clin Rheumatol. 2007. PMID: 17551382
-
ANA (+) ANCA (+) systemic vasculitis associated with the use of minocycline: case-based review.Clin Rheumatol. 2013 Jul;32(7):1099-106. doi: 10.1007/s10067-013-2245-z. Epub 2013 Apr 21. Clin Rheumatol. 2013. PMID: 23604593 Review.
-
Case report and review of minocycline-induced cutaneous polyarteritis nodosa.Arthritis Rheum. 2005 Jun 15;53(3):468-70. doi: 10.1002/art.21186. Arthritis Rheum. 2005. PMID: 15934105 Review. No abstract available.
Cited by
-
Spectrum of Large- and Medium-Vessel Vasculitis in Adults: Neoplastic, Infectious, Drug-Induced, Autoinflammatory, and Primary Immunodeficiency Diseases.Curr Rheumatol Rep. 2022 Oct;24(10):293-309. doi: 10.1007/s11926-022-01083-5. Epub 2022 Aug 3. Curr Rheumatol Rep. 2022. PMID: 35920952 Free PMC article. Review.
References
-
- Jennette JC, Falk RJ, Bacon PA, et al. . 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 65: 1-11, 2013. - PubMed
-
- Lhote F, Cohen P, Guillevin L. Polyarteritis nodosa, microscopic polyangiitis and Churg-Strauss syndrome. Lupus 7: 238-258, 1998. - PubMed
-
- Pagnoux C, Seror R, Henegar C, et al. . Clinical features and outcomes in 348 patients with polyarteritis nodosa: a systematic retrospective study of patients diagnosed between 1963 and 2005 and entered into the French Vasculitis Study Group Database. Arthritis Rheum 62: 616-626, 2010. - PubMed
-
- Selga D, Mohammad A, Sturfelt G, Segelmark M. Polyarteritis nodosa when applying the Chapel Hill nomenclature--a descriptive study on ten patients. Rheumatology (Oxford) 45: 1276-1281, 2006. - PubMed
-
- Hernández-Rodríguez J, Alba MA, Prieto-González S, Cid MC. Diagnosis and classification of polyarteritis nodosa. J Autoimmun 48-49: 84-89, 2014. - PubMed