

[Derivation and validation of a risk score for admission to the Intensive Care Unit in patients with COVID-19]
- PMID: 34176952
- PMCID: PMC8221018
- DOI: 10.1016/j.rce.2021.06.003
[Derivation and validation of a risk score for admission to the Intensive Care Unit in patients with COVID-19]
Abstract
Background: This work aims to identify and validate a risk scale for admission to intensive care units (ICU) in hospitalized patients with coronavirus disease 2019 (COVID-19).
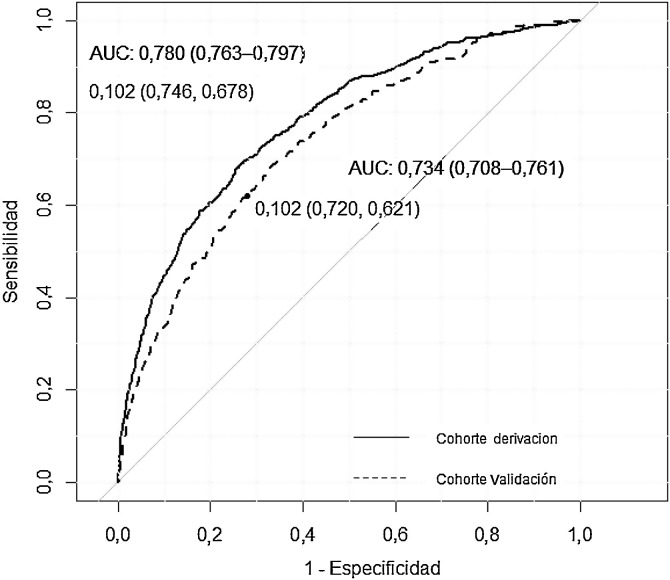
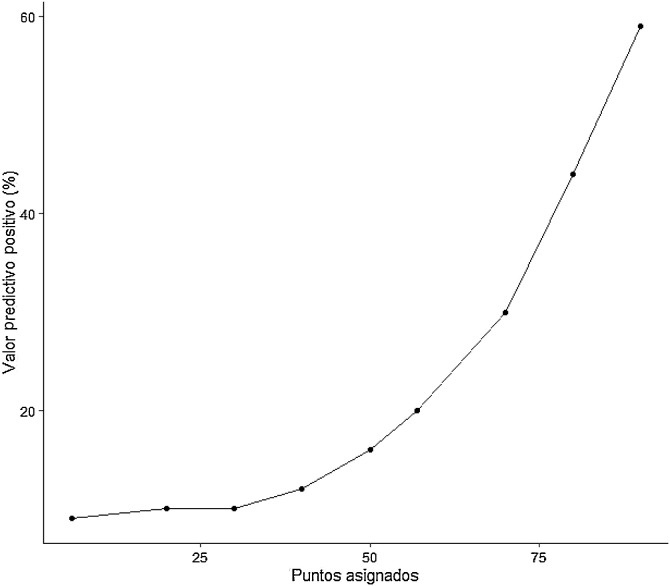
Methods: We created a derivation rule and a validation rule for ICU admission using data from a national registry of a cohort of patients with confirmed SARS-CoV-2 infection who were admitted between March and August 2020 (n = 16,298). We analyzed the available demographic, clinical, radiological, and laboratory variables recorded at hospital admission. We evaluated the performance of the risk score by estimating the area under the receiver operating characteristic curve (AUROC). Using the β coefficients of the regression model, we developed a score (0 to 100 points) associated with ICU admission.
Results: The mean age of the patients was 67 years; 57% were men. A total of 1,420 (8.7%) patients were admitted to the ICU. The variables independently associated with ICU admission were age, dyspnea, Charlson Comorbidity Index score, neutrophil-to-lymphocyte ratio, lactate dehydrogenase levels, and presence of diffuse infiltrates on a chest X-ray. The model showed an AUROC of 0.780 (CI: 0.763-0.797) in the derivation cohort and an AUROC of 0.734 (CI: 0.708-0.761) in the validation cohort. A score of greater than 75 points was associated with a more than 30% probability of ICU admission while a score of less than 50 points reduced the likelihood of ICU admission to 15%.
Conclusion: A simple prediction score was a useful tool for forecasting the probability of ICU admission with a high degree of precision.
Fundamento: Identificar y validar una escala de riesgo de ingreso en las unidades de cuidados intensivos (UCI) en pacientes hospitalizados con enfermedad por coronavirus 2019 (COVID-19).
Métodos: Realizamos una regla de derivación y otra de validación para ingreso en UCI, utilizando los datos de un registro nacional de cohortes de pacientes con infección confirmada por SARS-CoV-2 ingresados entre marzo y agosto del año 2020 (n = 16.298). Analizamos variables demográficas, clínicas, radiológicas y de laboratorio disponibles en el ingreso hospitalario. Evaluamos el rendimiento de la escala de riesgo mediante estimación del área bajo la curva de característica operativa del receptor (AROC). Utilizamos los coeficientes β del modelo de regresión para elaborar una puntuación (0 a 100 puntos) asociada con ingreso en UCI.
Resultados: La edad media de los pacientes fue de 67 años; 57% varones. Un total de 1.420 (8,7%) pacientes ingresaron en la UCI. Las variables independientes asociadas con el ingreso en UCI fueron: edad, disnea, índice de comorbilidad de Charlson, cociente neutrófilos-linfocitos, lactato deshidrogenasa e infiltrados difusos en la radiografía de tórax. El modelo mostró un AROC de 0,780 (IC: 0,763-0,797) en la cohorte de derivación y un AROC de 0,734 (IC: 0,708-0,761) en la cohorte de validación. Una puntuación > 75 se asoció con una probabilidad de ingreso en UCI superior a un 30%, mientras que una puntuación < 50 redujo la probabilidad de ingreso en UCI al 15%.
Conclusión: Una puntuación de predicción simple proporcionó una herramienta útil para predecir la probabilidad de ingreso en la UCI con un alto grado de precisión.
Keywords: Clinical epidemiology; Critical care; General linear model; Intensive care unit; Respiratory infection; Viral infection.
© 2021 Elsevier España, S.L.U. and Sociedad Española de Medicina Interna (SEMI). All rights reserved.
Figures
Similar articles
-
Derivation and validation of a risk score for admission to the Intensive Care Unit in patients with COVID-19.Rev Clin Esp (Barc). 2022 Jan;222(1):1-12. doi: 10.1016/j.rceng.2021.06.001. Epub 2021 Sep 14. Rev Clin Esp (Barc). 2022. PMID: 34561194 Free PMC article.
-
Predictive value of National Early Warning Score 2 (NEWS2) for intensive care unit admission in patients with SARS-CoV-2 infection.Infect Dis (Lond). 2020 Oct;52(10):698-704. doi: 10.1080/23744235.2020.1784457. Epub 2020 Jun 25. Infect Dis (Lond). 2020. PMID: 32584161
-
Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19.JAMA Intern Med. 2020 Aug 1;180(8):1081-1089. doi: 10.1001/jamainternmed.2020.2033. JAMA Intern Med. 2020. PMID: 32396163 Free PMC article.
-
Factors Associated with ICU Admission in Patients with COVID-19: The GOL2DS Score.Medicina (Kaunas). 2021 Dec 12;57(12):1356. doi: 10.3390/medicina57121356. Medicina (Kaunas). 2021. PMID: 34946301 Free PMC article.
-
Development and Validation of a Multivariable Predictive Model for Mortality of COVID-19 Patients Demanding High Oxygen Flow at Admission to ICU: AIDA Score.Oxid Med Cell Longev. 2021 Jun 30;2021:6654388. doi: 10.1155/2021/6654388. eCollection 2021. Oxid Med Cell Longev. 2021. PMID: 34257816 Free PMC article. Clinical Trial.
Cited by
-
[Predicting COVID-19 progress with clinical scales].Rev Clin Esp. 2022 Jan;222(1):42-43. doi: 10.1016/j.rce.2021.08.001. Epub 2021 Sep 1. Rev Clin Esp. 2022. PMID: 34483348 Free PMC article. Spanish. No abstract available.
-
Predicting COVID-19 progress with clinical scales.Rev Clin Esp (Barc). 2022 Jan;222(1):42-43. doi: 10.1016/j.rceng.2021.08.001. Epub 2021 Oct 21. Rev Clin Esp (Barc). 2022. PMID: 34756571 Free PMC article. No abstract available.
References
-
- Secretaría de Estado de Sanidad/Centro de Coordinación de Alertas y Emergencias Sanitarias. Actualización n° 355. Enfermedad por el coronavirus (COVID-19). [Consultado 14 Abr 2021]. Disponible en: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual...
-
- Ferrando C., Mellado-Artigas R., Gea A., Arruti E., Aldecoa C., Bordell A., et al. Patient characteristics, clinical course and factors associated to ICU mortality in critically ill patients infected with SARS-CoV-2 in Spain: A prospective, cohort, multicentre study. Rev Esp Anestesiol Reanim. 2020;67:425–437. doi: 10.1016/j.redar.2020.07.003. Epub 2020 Jul 13. PMID: 32800622; PMCID: PMC7357496. - PMC - PubMed
-
- Berenguer J., Ryan P., Rodríguez-Baño J., Jarrín I., Carratalà J., Pachón J., et al. Characteristics and predictors of death among 4035 consecutively hospitalized patients with COVID-19 in Spain. Clin Microbiol Infect. 2020;26:1525–1536. doi: 10.1016/j.cmi.2020.07.024. Epub 2020 Aug 4. PMID: 32758659; PMCID: PMC7399713. - DOI - PMC - PubMed
-
- Núñez-Gil I.J., Fernández-Pérez C., Estrada V., Becerra-Muñoz V.M., El-Battrawy I., Uribarri A., et al. Mortality risk assessment in Spain and Italy, insights of the HOPE COVID-19 registry. Intern Emerg Med. 2021;16:957–966. doi: 10.1007/s11739-020-02543-5. PMID: 33165755; PMCID: PMC7649104. - DOI - PMC - PubMed
