

Ethical Issues and Management of Fetal Hemolytic Anemia Caused by Anti-Rh17 in a Multipara with Rare -D- Phenotype
- PMID: 34177424
- PMCID: PMC8216032
- DOI: 10.1159/000513124
Ethical Issues and Management of Fetal Hemolytic Anemia Caused by Anti-Rh17 in a Multipara with Rare -D- Phenotype
Abstract
Background: The development of allo-anti-Rh17 (anti-Hr0) in a -D- phenotype whose red blood cells (RBCs) lack CcEe antigens is most likely triggered by transfusion, transplantation, or pregnancy. Gene conversion is the predominating factor in generating RHD-CE-D and RHCE-D-CE hybrids like -D-.
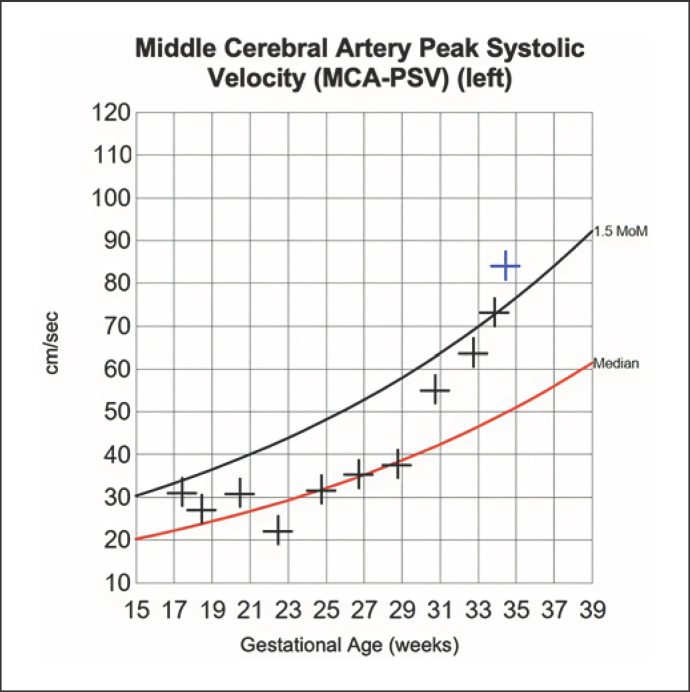
Methods: We report here immunohematological and obstetrical data from 2 of the 5 pregnancies of a 24-year-old woman presenting with the -D- phenotype with anti-Rh17. Blood group typing, antibody screening, antibody differentiation, direct antiglobulin test (DAT), and antibody titers were performed by routine gel technology and tube testing. Additionally, molecular genetic analysis was performed. Fetal surveillance was done by sonographic evaluation of the fetal middle cerebral artery peak systolic velocity (MCA-PSV).
Results: Blood group typing showed O, C-c-D+E-e- and the DAT was negative. DNA sequencing revealed homozygosity for an RHCE-D(3-9)-CE null allele. Anti-Rh17 titers in the fourth pregnancy remained between 1:8 and 1:128, and no signs for a fetal anemia were observed. However, in the fifth pregnancy, the antibody titers increased up to 1:4,096. Signs of moderate fetal anemia were detected and cesarean section was performed at 34 + 6 weeks of gestation. The newborn presented with hemolytic anemia (cord blood hemoglobin [Hb] = 8.5 mg/dL). She received 2 compatible (small) packed RBC concentrates, phototherapy, and intravenous immunoglobulins.
Conclusion: Our case shows that the risk for hemolytic complications increases with the number of pregnancies of sensitized women. Only people who also lack CcEe antigens are compatible as donors. The role of such rare donors as lifesavers, their freedom, and voluntariness conflict with the urgent need for compatible blood.
Keywords: Anti-Rh17 (anti-Hr0); Hemolytic anemia; Hyperbilirubinemia; Maternal alloimmunization; Medical ethics.
Copyright © 2021 by S. Karger AG, Basel.
Conflict of interest statement
The authors declare that they have no conflicts of interest relevant to the manuscript.
Figures
Similar articles
-
Fetal hemolytic disease due to anti-Rh17 alloimmunization.Fetal Diagn Ther. 2004 Mar-Apr;19(2):182-6. doi: 10.1159/000075147. Fetal Diagn Ther. 2004. PMID: 14764967 Review.
-
The Outcome of Hemolytic Disease of the Fetus and Newborn Caused by Anti-Rh17 Antibody: Analysis of Three Cases and Review of the Literature.Transfus Med Hemother. 2020 Jun;47(3):264-271. doi: 10.1159/000503012. Epub 2019 Oct 3. Transfus Med Hemother. 2020. PMID: 32595431 Free PMC article. Review.
-
Recurrent pregnancy loss in a patient with anti-Rh17.Transfus Med. 2024 Feb;34(1):66-70. doi: 10.1111/tme.13014. Epub 2023 Nov 8. Transfus Med. 2024. PMID: 37941301
-
Successful management of fetal hemolytic disease due to strong anti-Rh17 with plasma exchange and intrauterine transfusion in a woman with the D-- phenotype.Int J Hematol. 2020 Jan;111(1):149-154. doi: 10.1007/s12185-019-02735-6. Epub 2019 Sep 19. Int J Hematol. 2020. PMID: 31538326
-
Maternal ABO-mismatched blood for intrauterine transfusion of severe hemolytic disease of the newborn due to anti-Rh17.Transfusion. 2004 Sep;44(9):1357-60. doi: 10.1111/j.1537-2995.2004.04082.x. Transfusion. 2004. PMID: 15318861
Cited by
-
Characterization of Novel RHD Allele Variants and Their Implications for Routine Blood Group Diagnostics.Biomedicines. 2024 Feb 18;12(2):456. doi: 10.3390/biomedicines12020456. Biomedicines. 2024. PMID: 38398058 Free PMC article.
-
Integrated analyses reveal unexpected complex inversion and recombination in RH genes.Blood Adv. 2024 Jun 25;8(12):3154-3165. doi: 10.1182/bloodadvances.2023012147. Blood Adv. 2024. PMID: 38551808 Free PMC article.
References
-
- Daniels G. Human Blood Groups. 3rd ed. Wiley-Blackwell; 2013.
-
- Denomme GA, Ryan G, Seaward PG, Kelly EN, Fernandes BJ. Maternal ABO-mismatched blood for intrauterine transfusion of severe hemolytic disease of the newborn due to anti-Rh17. Transfusion. 2004 Sep;44((9)):1357–60. - PubMed
-
- Aref K, Boctor FN, Pande S, Uehlinger J, Manning F, Eglowstein M, et al. Successful perinatal management of hydrops fetalis due to hemolytic disease associated with D— maternal phenotype. J Perinatol. 2002 Dec;22((8)):667–8. - PubMed
-
- Hirose M, Nakanishi K, Kaku S, Moro H, Hodohara K, Aotani H, et al. Fetal hemolytic disease due to anti-Rh17 alloimmunization. Fetal Diagn Ther. 2004 Mar-Apr;19((2)):182–6. - PubMed
-
- Li BJ, Jiang YJ, Yuan F, Ye HX. Exchange transfusion of least incompatible blood for severe hemolytic disease of the newborn due to anti-Rh17. Transfus Med. 2010 Feb;20((1)):66–9. - PubMed
LinkOut - more resources
Full Text Sources
