

Metastatic Prostate Cancer Synchronous with Male Breast Papillary Ductal Carcinoma in situ: Management Dilemma and Literature Review
- PMID: 34177531
- PMCID: PMC8215967
- DOI: 10.1159/000515784
Metastatic Prostate Cancer Synchronous with Male Breast Papillary Ductal Carcinoma in situ: Management Dilemma and Literature Review
Abstract
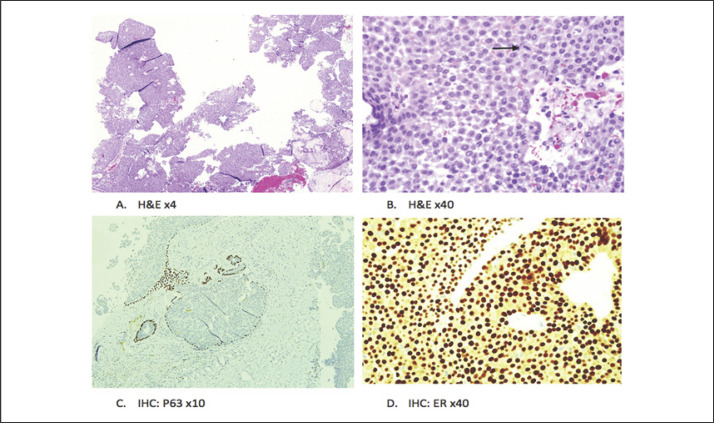
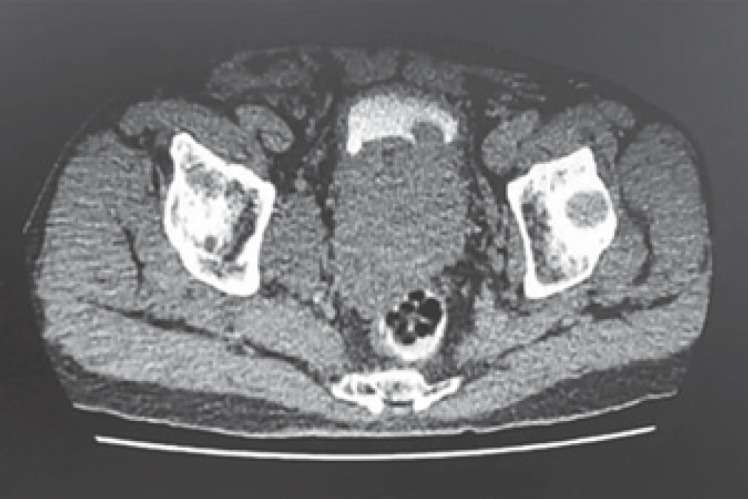
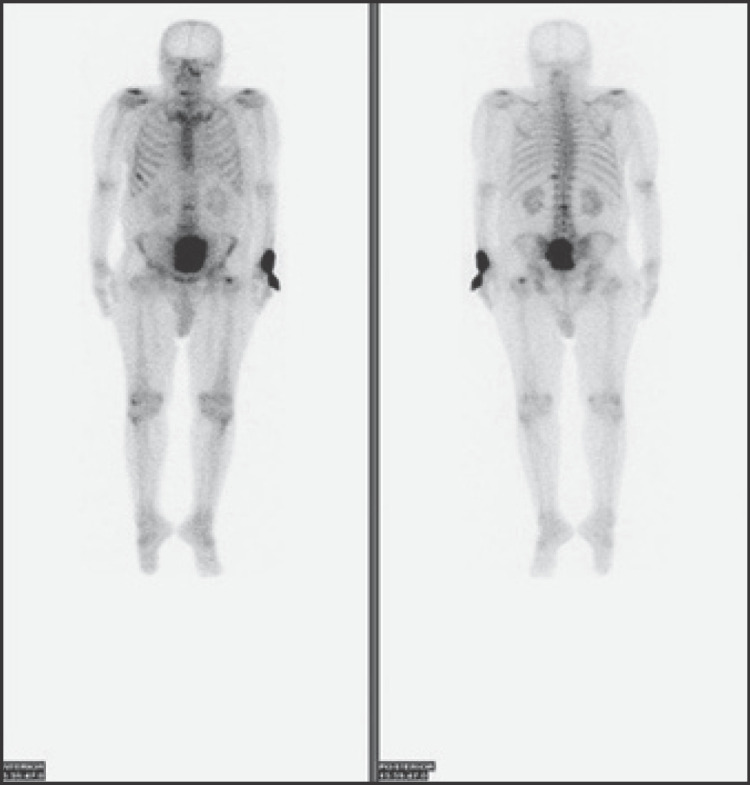
Prostate cancer is common in men, but tumour of the male breast is rare. For these two tumours to be presented synchronously in a male patient is even rarer. The focus of this paper is the case of a 72-year-old man diagnosed with papillary ductal carcinoma in situ after he presented with a unilateral breast mass associated with nipple discharge. Imaging staging for his breast tumour and subsequent prostate biopsy found an incidental synchronous asymptomatic prostate adenocarcinoma as well as bone metastases. He denies risk factors for malignancies and refuses genetic testing. The first part of our discussion will highlight the uncommon occurrence of male breast ductal carcinoma in situ and its management controversies. The subsequent part of our discussion will focus on the association between male breast cancer and prostate cancer, and implication of this on the future treatment of these patients. More importantly, our case will illustrate the challenges in managing dual primaries that present concurrently.
Keywords: Ductal carcinoma in situ; Male breast; Prostate cancer; Synchronous.
Copyright © 2021 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Synchronous bilateral noninvasive ductal carcinoma of the male breast: a case report.Breast Cancer. 2003;10(2):163-6. doi: 10.1007/BF02967643. Breast Cancer. 2003. PMID: 12736571 Review.
-
Magnetic resonance imaging findings of high-grade ductal carcinoma in situ of the male breast: A case report.SAGE Open Med Case Rep. 2018 Jun 12;6:2050313X18781727. doi: 10.1177/2050313X18781727. eCollection 2018. SAGE Open Med Case Rep. 2018. PMID: 29977557 Free PMC article.
-
Ductal Carcinoma In situ of the Male Breast.Breast Care (Basel). 2016 Aug;11(4):288-290. doi: 10.1159/000447768. Epub 2016 Aug 5. Breast Care (Basel). 2016. PMID: 27721718 Free PMC article.
-
A Synchronous Diagnosis of Metastatic Male Breast Cancer and Prostate Cancer.J Investig Med High Impact Case Rep. 2019 Jan-Dec;7:2324709619847230. doi: 10.1177/2324709619847230. J Investig Med High Impact Case Rep. 2019. PMID: 31053047 Free PMC article.
-
Papillary carcinoma of the breast in a male patient with a treated prostatic carcinoma diagnosed by fine-needle aspiration biopsy: a case report and review of the literature.Diagn Cytopathol. 2006 Mar;34(3):214-7. doi: 10.1002/dc.20402. Diagn Cytopathol. 2006. PMID: 16548002 Free PMC article. Review.
Cited by
-
Profile of Male Breast Cancer in Makkah Region of Saudi Arabia: A 4-Year Retrospective Analysis of Radiology and Histopathology.Int J Breast Cancer. 2022 Jun 22;2022:8831011. doi: 10.1155/2022/8831011. eCollection 2022. Int J Breast Cancer. 2022. PMID: 35784659 Free PMC article.
References
-
- Culp MB, Soerjomataram I, Efstathiou JA, Bray F, Jemal A. Recent global patterns in prostate cancer incidence and mortality rates. Eur Urol. 2020 Jan 1;77((1)):38–52. - PubMed
-
- Liu N, Johnson KJ, Ma CX. Male breast cancer: an updated surveillance, epidemiology, and end results data analysis. Clin Breast Cancer. 2018 Oct 1;18((5)):e997–1002. - PubMed
-
- Giordano SH. Breast cancer in men. N Engl J Med. 2018 Jun 14;378((24)):2311–20. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
