

Postoperative Macular Proliferative Vitreoretinopathy: A Case Series and Literature Review
- PMID: 34177543
- PMCID: PMC8215993
- DOI: 10.1159/000512285
Postoperative Macular Proliferative Vitreoretinopathy: A Case Series and Literature Review
Abstract
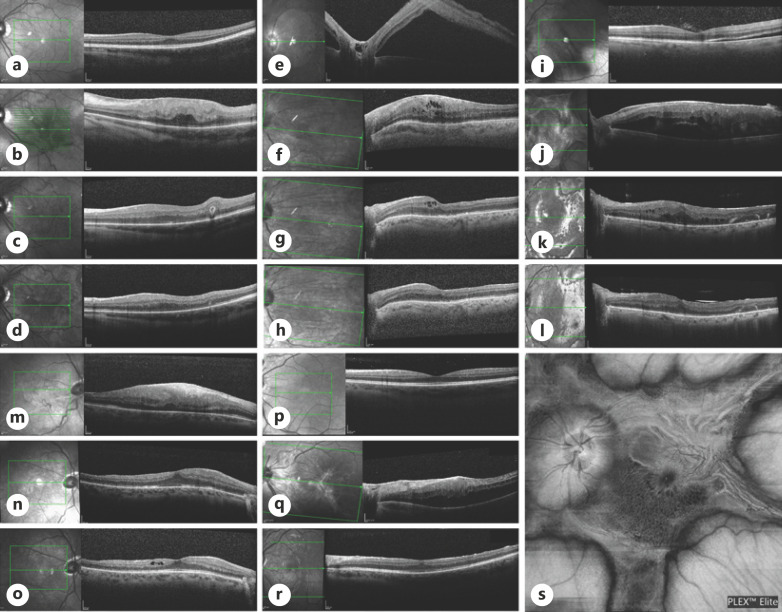
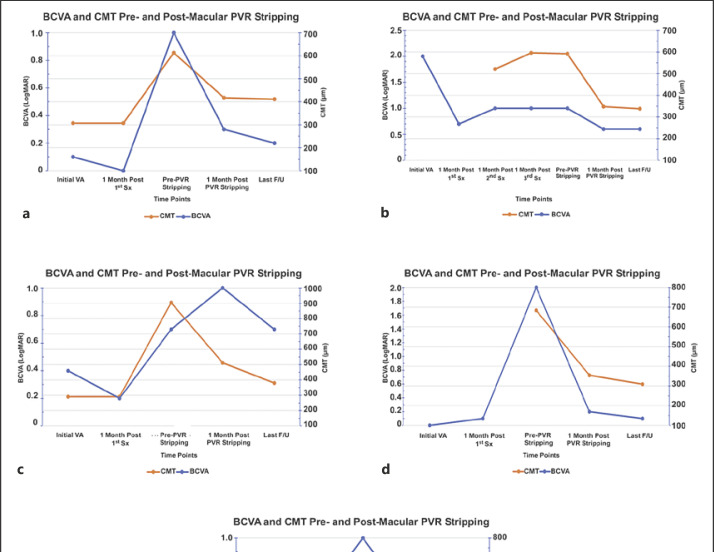
Premacular membranes developing following pars plana vitrectomy (PPV) can cause significant anatomical and functional deficits to the macula. Recent reports showed that postoperative premacular membranes are a localized presentation of macular proliferative vitreoretinopathy (mPVR). Here, we report retrospectively a case series of 5 patients with severe mPVR which developed following uneventful PPV and were followed up to 32 months in the Department of Ophthalmology, Hadassah-Hebrew University Medical Center, Jerusalem, between October 2016 and February 2020. All patients underwent primary repair of rhegmatogenous retinal detachment (RRD) before mPVR developed. Mean best-corrected visual acuity (BCVA) at presentation was 20/76 Snellen (0.58 LogMAR). Median duration of the retinal detachment time until surgery was 1.5 days (range 1-21 days). Mean interval time from last normal follow-up exam to diagnosis of mPVR was 19 days (range 10-28). BCVA dropped from a mean of 20/38 Snellen (0.28 LogMAR) prior to mPVR development to 20/166 Snellen (0.92 LogMAR) following its development, recovering to 20/57 Snellen (0.45 LogMAR) after peeling of membranes. Mean central macular thickness measured by optical coherence tomography decreased from 711 to 354 μm postsurgery. In conclusion, short-term mPVR is a different entity from macular pucker in terms of rapid development, structural distortion, and visual compromise. Surgical treatment significantly restores macular function and anatomy.
Keywords: Epiretinal membrane; Macular proliferative vitreoretinopathy; Macular pucker; Post-operative; Premacular membrane.
Copyright © 2021 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- Sigler EJ, Randolph JC, Calzada JI. Comparison of morphologic features of macular proliferative vitreoretinopathy and idiopathic epimacular membrane. Retina. 2014;34((8)):1651–7. - PubMed
-
- Guenther SR, Schumann RG, Hagenau F, Wolf A, Priglinger SG, Vogt D. Comparison of surgically excised premacular membranes in eyes with macular pucker and proliferative vitreoretinopathy. Curr Eye Res. 2019;44((3)):341–9. - PubMed
-
- Pastor JC, De La Rúa ER, Martín F. Proliferative vitreoretinopathy: risk factors and pathobiology. Prog Retin Eye Res. 2002;21:127–44. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
