

Analysis of Prognostic Risk Factors Determining Poor Functional Recovery After Comprehensive Rehabilitation Including Motor-Imagery Brain-Computer Interface Training in Stroke Patients: A Prospective Study
- PMID: 34177767
- PMCID: PMC8222567
- DOI: 10.3389/fneur.2021.661816
Analysis of Prognostic Risk Factors Determining Poor Functional Recovery After Comprehensive Rehabilitation Including Motor-Imagery Brain-Computer Interface Training in Stroke Patients: A Prospective Study
Abstract
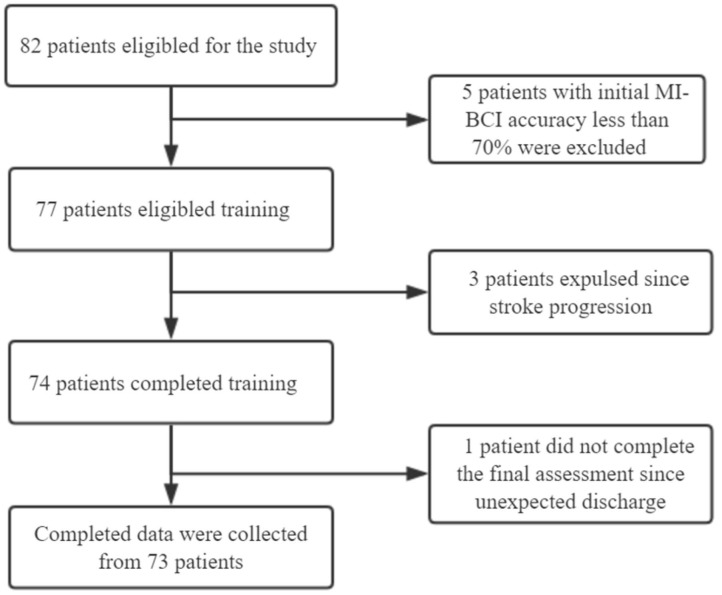
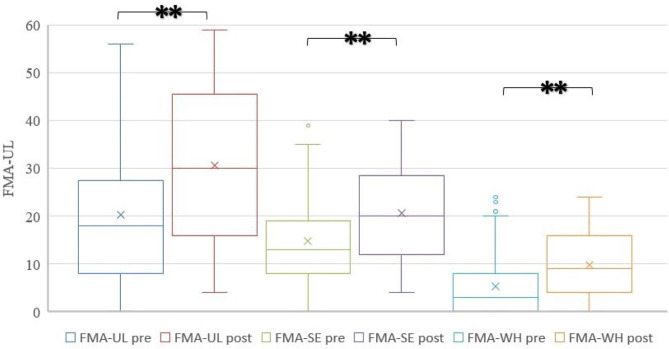
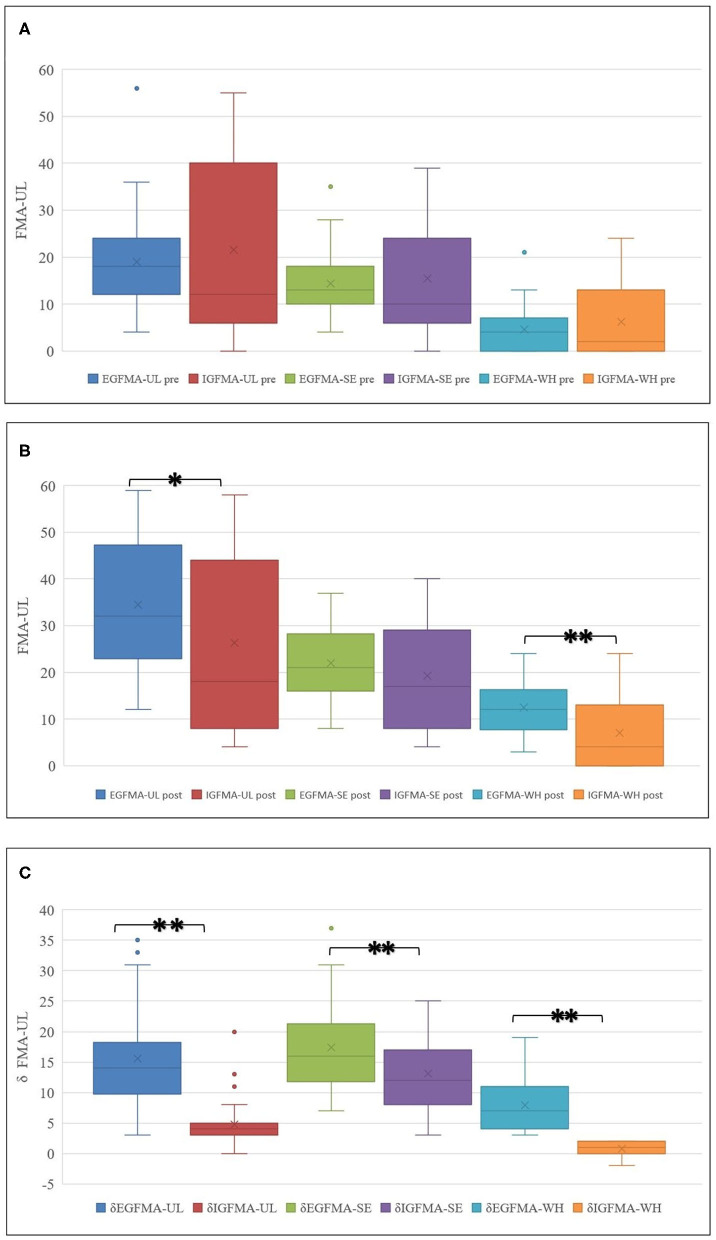
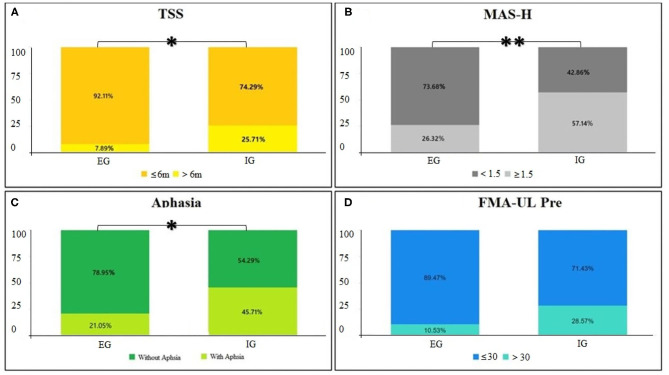
Objective: Upper limb (UL) motor function recovery, especially distal function, is one of the main goals of stroke rehabilitation as this function is important to perform activities of daily living (ADL). The efficacy of the motor-imagery brain-computer interface (MI-BCI) has been demonstrated in patients with stroke. Most patients with stroke receive comprehensive rehabilitation, including MI-BCI and routine training. However, most aspects of MI-BCI training for patients with subacute stroke are based on routine training. Risk factors for inadequate distal UL functional recovery in these patients remain unclear; therefore, it is more realistic to explore the prognostic factors of this comprehensive treatment based on clinical practice. The present study aims to investigate the independent risk factors that might lead to inadequate distal UL functional recovery in patients with stroke after comprehensive rehabilitation including MI-BCI (CRIMI-BCI). Methods: This prospective study recruited 82 patients with stroke who underwent CRIMI-BCI. Motor-imagery brain-computer interface training was performed for 60 min per day, 5 days per week for 4 weeks. The primary outcome was improvement of the wrist and hand dimensionality of Fugl-Meyer Assessment (δFMA-WH). According to the improvement score, the patients were classified into the efficient group (EG, δFMA-WH > 2) and the inefficient group (IG, δFMA-WH ≤ 2). Binary logistic regression was used to analyze clinical and demographic data, including aphasia, spasticity of the affected hand [assessed by Modified Ashworth Scale (MAS-H)], initial UL function, age, gender, time since stroke (TSS), lesion hemisphere, and lesion location. Results: Seventy-three patients completed the study. After training, all patients showed significant improvement in FMA-UL (Z = 7.381, p = 0.000**), FMA-SE (Z = 7.336, p = 0.000**), and FMA-WH (Z = 6.568, p = 0.000**). There were 35 patients (47.9%) in the IG group and 38 patients (52.1%) in the EG group. Multivariate analysis revealed that presence of aphasia [odds ratio (OR) 4.617, 95% confidence interval (CI) 1.435-14.860; p < 0.05], initial FMA-UL score ≤ 30 (OR 5.158, 95% CI 1.150-23.132; p < 0.05), and MAS-H ≥ level I+ (OR 3.810, 95% CI 1.231-11.790; p < 0.05) were the risk factors for inadequate distal UL functional recovery in patients with stroke after CRIMI-BCI. Conclusion: We concluded that CRIMI-BCI improved UL function in stroke patients with varying effectiveness. Inferior initial UL function, significant hand spasticity, and presence of aphasia were identified as independent risk factors for inadequate distal UL functional recovery in stroke patients after CRIMI-BCI.
Keywords: motor-imagery brain-computer interface; regression analysis; rehabilitation; stroke; upper limb.
Copyright © 2021 Wu, Ge, Ma, Pang, Cao, Zhang, Pan, Zhang and Dou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Brain Functional Networks Study of Subacute Stroke Patients With Upper Limb Dysfunction After Comprehensive Rehabilitation Including BCI Training.Front Neurol. 2020 Jan 27;10:1419. doi: 10.3389/fneur.2019.01419. eCollection 2019. Front Neurol. 2020. PMID: 32082238 Free PMC article.
-
SSVEP-Based Brain Computer Interface Controlled Soft Robotic Glove for Post-Stroke Hand Function Rehabilitation.IEEE Trans Neural Syst Rehabil Eng. 2022;30:1737-1744. doi: 10.1109/TNSRE.2022.3185262. Epub 2022 Jul 4. IEEE Trans Neural Syst Rehabil Eng. 2022. PMID: 35731756 Clinical Trial.
-
The Promotoer, a brain-computer interface-assisted intervention to promote upper limb functional motor recovery after stroke: a study protocol for a randomized controlled trial to test early and long-term efficacy and to identify determinants of response.BMC Neurol. 2020 Jun 27;20(1):254. doi: 10.1186/s12883-020-01826-w. BMC Neurol. 2020. PMID: 32593293 Free PMC article.
-
Effects of brain-computer interface based training on post-stroke upper-limb rehabilitation: a meta-analysis.J Neuroeng Rehabil. 2025 Mar 3;22(1):44. doi: 10.1186/s12984-025-01588-x. J Neuroeng Rehabil. 2025. PMID: 40033447 Free PMC article. Review.
-
Effect of brain-computer interface training based on non-invasive electroencephalography using motor imagery on functional recovery after stroke - a systematic review and meta-analysis.BMC Neurol. 2020 Oct 22;20(1):385. doi: 10.1186/s12883-020-01960-5. BMC Neurol. 2020. PMID: 33092554 Free PMC article.
Cited by
-
A Cross-Sectional Study: Determining Factors of Functional Independence and Quality of Life of Patients One Month after Having Suffered a Stroke.Int J Environ Res Public Health. 2023 Jan 5;20(2):995. doi: 10.3390/ijerph20020995. Int J Environ Res Public Health. 2023. PMID: 36673749 Free PMC article.
References
-
- Woytowicz EJ, Rietschel JC, Goodman RN, Conroy SS, Sorkin JD, Whitall J, et al. . Determining levels of upper extremity movement impairment by applying a cluster analysis to the Fugl-Meyer assessment of the upper extremity in chronic stroke. Arch Phys Med Rehabil. (2017) 98:456–62. 10.1016/j.apmr.2016.06.023 - DOI - PMC - PubMed
-
- Carino-Escobar RI, Carrillo-Mora P, Valdés-Cristerna R, Rodriguez-Barragan MA, Hernandez-Arenas C, Quinzaños-Fresnedo J, et al. . Longitudinal analysis of stroke patients' brain rhythms during an intervention with a brain-computer interface. Neural Plast. (2019) 2019:1–11. 10.1155/2019/7084618 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources