

Safety and Efficacy of Low-Dose Tirofiban Combined With Intravenous Thrombolysis and Mechanical Thrombectomy in Acute Ischemic Stroke: A Matched-Control Analysis From a Nationwide Registry
- PMID: 34177774
- PMCID: PMC8225265
- DOI: 10.3389/fneur.2021.666919
Safety and Efficacy of Low-Dose Tirofiban Combined With Intravenous Thrombolysis and Mechanical Thrombectomy in Acute Ischemic Stroke: A Matched-Control Analysis From a Nationwide Registry
Abstract
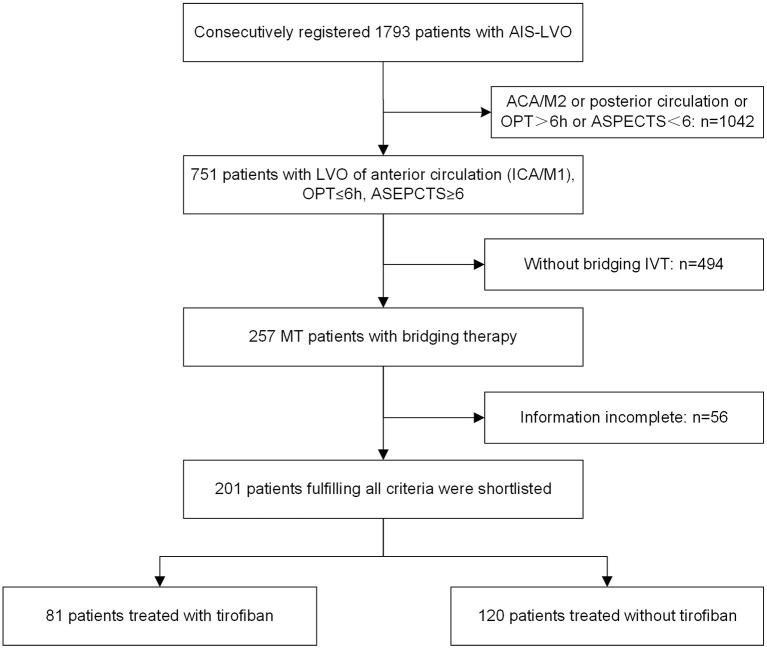
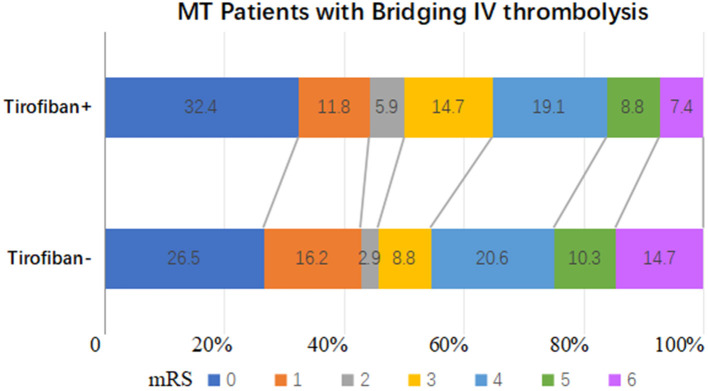
Purpose: Tirofiban administration to acute ischemic stroke patients undergoing mechanical thrombectomy with preceding intravenous thrombolysis remains controversial. The aim of the current study was to evaluate the safety and efficacy of low-dose tirofiban during mechanical thrombectomy in patients with preceding intravenous thrombolysis. Methods: Patients with acute ischemic stroke undergoing mechanical thrombectomy and preceding intravenous thrombolysis were derived from "ANGEL-ACT," a multicenter, prospective registry study. The patients were dichotomized into tirofiban and non-tirofiban groups based on whether tirofiban was administered. Propensity score matching was used to minimize case bias. The primary safety endpoint was symptomatic intracerebral hemorrhage (sICH), defined as an intracerebral hemorrhage (ICH) associated with clinical deterioration as determined by the Heidelberg Bleeding Classification. All ICHs and hemorrhage types were recorded. Clinical outcomes included successful recanalization, dramatic clinical improvement, functional independence, and mortality at the 3-month follow-up timepoint. Successful recanalization was defined as a modified Thrombolysis in Cerebral Ischemia score of 2b or 3. Dramatic clinical improvement at 24 h was defined as a reduction in NIH stroke score of ≥10 points compared with admission, or a score ≤1. Functional independence was defined as a Modified Rankin Scale (mRS) score of 0-2 at 3-months. Results: The study included 201 patients, 81 in the tirofiban group and 120 in the non-tirofiban group, and each group included 68 patients after propensity score matching. Of the 201 patients, 52 (25.9%) suffered ICH, 15 (7.5%) suffered sICH, and 18 (9.0%) died within 3-months. The median mRS was 3 (0-4), 99 (49.3%) achieved functional independence. There were no statistically significant differences in safety outcomes, efficacy outcomes on successful recanalization, dramatic clinical improvement, or 3-month mRS between the tirofiban and non-tirofiban groups (all p > 0.05). Similar results were obtained after propensity score matching. Conclusion: In acute ischemic stroke patients who underwent mechanical thrombectomy and preceding intravenous thrombolysis, low-dose tirofiban was not associated with increased risk of sICH or ICH. Further randomized clinical trials are needed to confirm the effects of tirofiban in patients undergoing bridging therapy.
Keywords: intravenous thrombolysis; large vessel occlusion; mechanical thrombectomy; propensity score matching; tirofiban.
Copyright © 2021 Ma, Li, Jia, Mo, Ma, Gao, Huo, Luo, Wang, Pan, Song, Sun, Zhang, Gui, Song, Peng, Wu, Zhao, Zhao, Zhou and Miao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer WZ declared a shared affiliation, with no collaboration with several of the authors to the handling Editor.
Figures
Similar articles
-
Safety and Efficacy of Tirofiban During Intravenous Thrombolysis Bridging to Mechanical Thrombectomy for Acute Ischemic Stroke Patients: A Meta-Analysis.Front Neurol. 2022 Apr 29;13:851910. doi: 10.3389/fneur.2022.851910. eCollection 2022. Front Neurol. 2022. PMID: 35572929 Free PMC article.
-
Safety and Efficacy of Tirofiban During Mechanical Thrombectomy for Stroke Patients with Preceding Intravenous Thrombolysis.Clin Interv Aging. 2020 Jul 23;15:1241-1248. doi: 10.2147/CIA.S238769. eCollection 2020. Clin Interv Aging. 2020. PMID: 32801672 Free PMC article.
-
Intravenous Administration of Standard Dose Tirofiban after Mechanical Arterial Recanalization is Safe and Relatively Effective in Acute Ischemic Stroke.Aging Dis. 2019 Oct 1;10(5):1049-1057. doi: 10.14336/AD.2018.0922. eCollection 2019 Oct. Aging Dis. 2019. PMID: 31595202 Free PMC article.
-
Safety and efficacy of intravenous Tirofiban infusion after mechanical thrombectomy in acute ischemic stroke: a retrospective observational study.Am J Transl Res. 2021 Aug 15;13(8):9076-9085. eCollection 2021. Am J Transl Res. 2021. PMID: 34540021 Free PMC article.
-
Early tirofiban administration for patients with acute ischemic stroke treated with intravenous thrombolysis or bridging therapy: Systematic review and meta-analysis.Clin Neurol Neurosurg. 2022 Nov;222:107449. doi: 10.1016/j.clineuro.2022.107449. Epub 2022 Sep 21. Clin Neurol Neurosurg. 2022. PMID: 36162161
Cited by
-
Prospective pilot study of tirofiban in progressive stroke after intravenous thrombolysis.Front Neurol. 2022 Oct 4;13:982684. doi: 10.3389/fneur.2022.982684. eCollection 2022. Front Neurol. 2022. PMID: 36267890 Free PMC article.
-
Conservative versus aggressive antiplatelet strategy for emergent carotid stenting during stroke thrombectomy.Interv Neuroradiol. 2023 Jun;29(3):268-276. doi: 10.1177/15910199221083112. Epub 2022 Mar 7. Interv Neuroradiol. 2023. PMID: 35253529 Free PMC article.
-
Safety and efficacy of different tirofiban administration routes on acute ischemic stroke patients with successful recanalization: A propensity score matching analysis.CNS Neurosci Ther. 2022 Dec;28(12):1993-2000. doi: 10.1111/cns.13936. Epub 2022 Aug 13. CNS Neurosci Ther. 2022. PMID: 35962605 Free PMC article.
-
Modular-Based Synergetic Mechanisms of Jasminoidin and Ursodeoxycholic Acid in Cerebral Ischemia Therapy.Biomedicines. 2025 Apr 11;13(4):938. doi: 10.3390/biomedicines13040938. Biomedicines. 2025. PMID: 40299522 Free PMC article.
-
Safety and Efficacy of Tirofiban During Intravenous Thrombolysis Bridging to Mechanical Thrombectomy for Acute Ischemic Stroke Patients: A Meta-Analysis.Front Neurol. 2022 Apr 29;13:851910. doi: 10.3389/fneur.2022.851910. eCollection 2022. Front Neurol. 2022. PMID: 35572929 Free PMC article.
References
LinkOut - more resources
Full Text Sources