

Sarcoidosis-lymphoma syndrome with portal hypertension: diagnostic clues and approach
- PMID: 34178191
- PMCID: PMC8213984
- DOI: 10.1016/j.radcr.2021.05.045
Sarcoidosis-lymphoma syndrome with portal hypertension: diagnostic clues and approach
Abstract
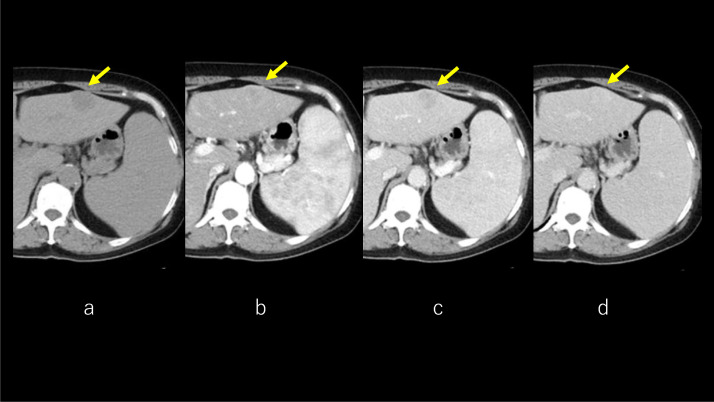
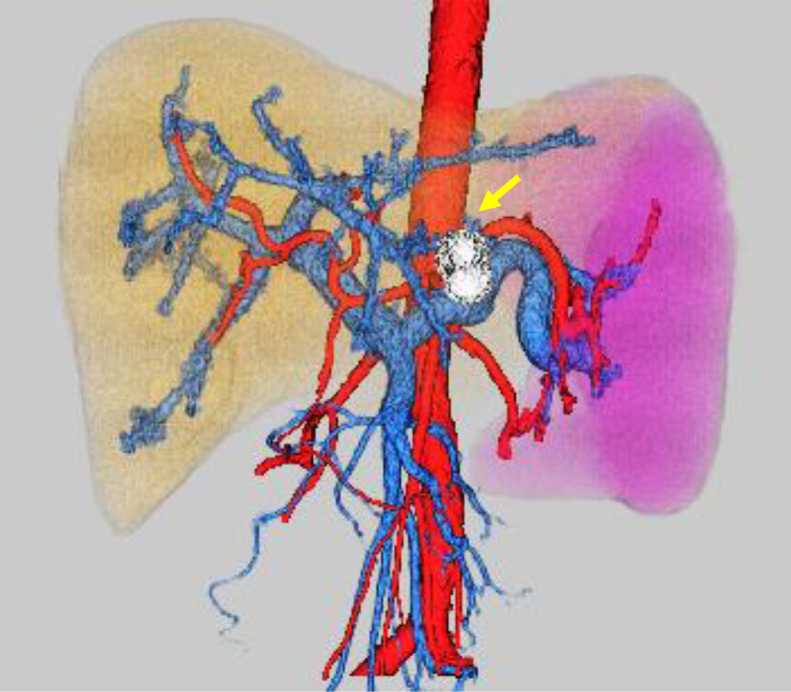
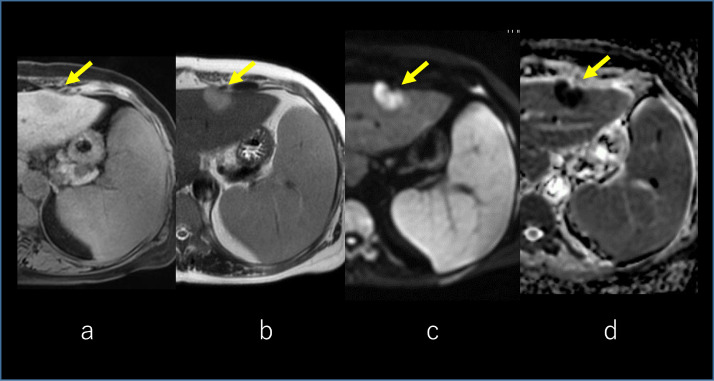
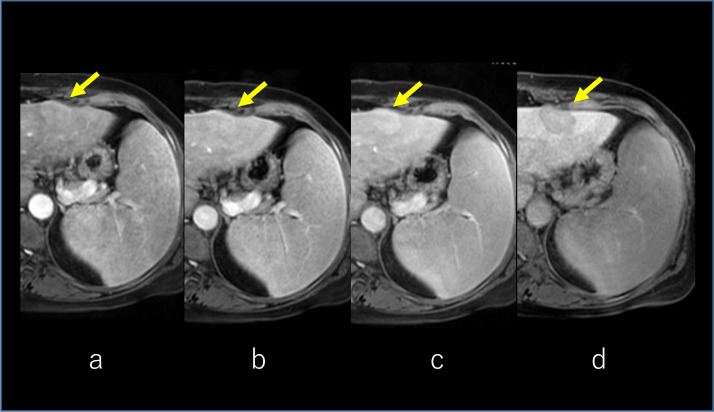
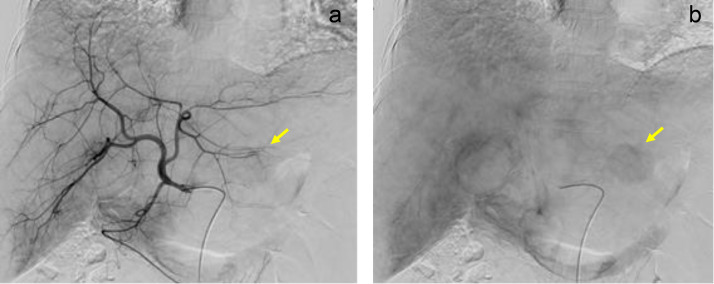
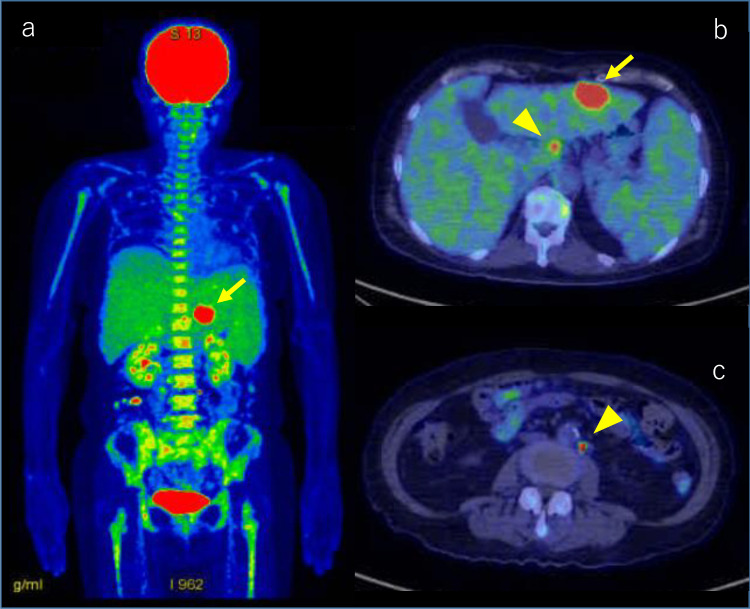
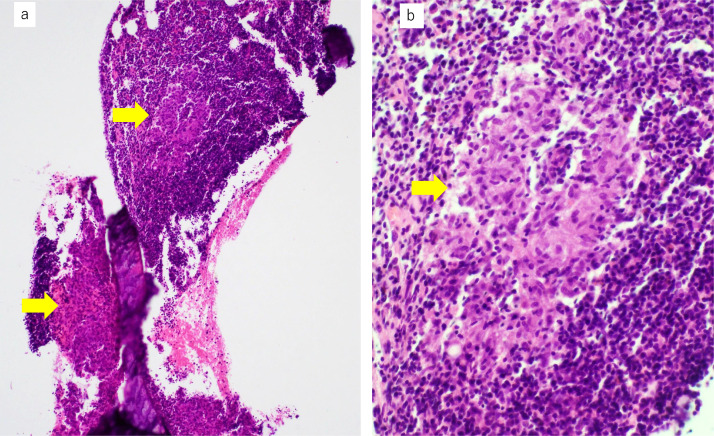
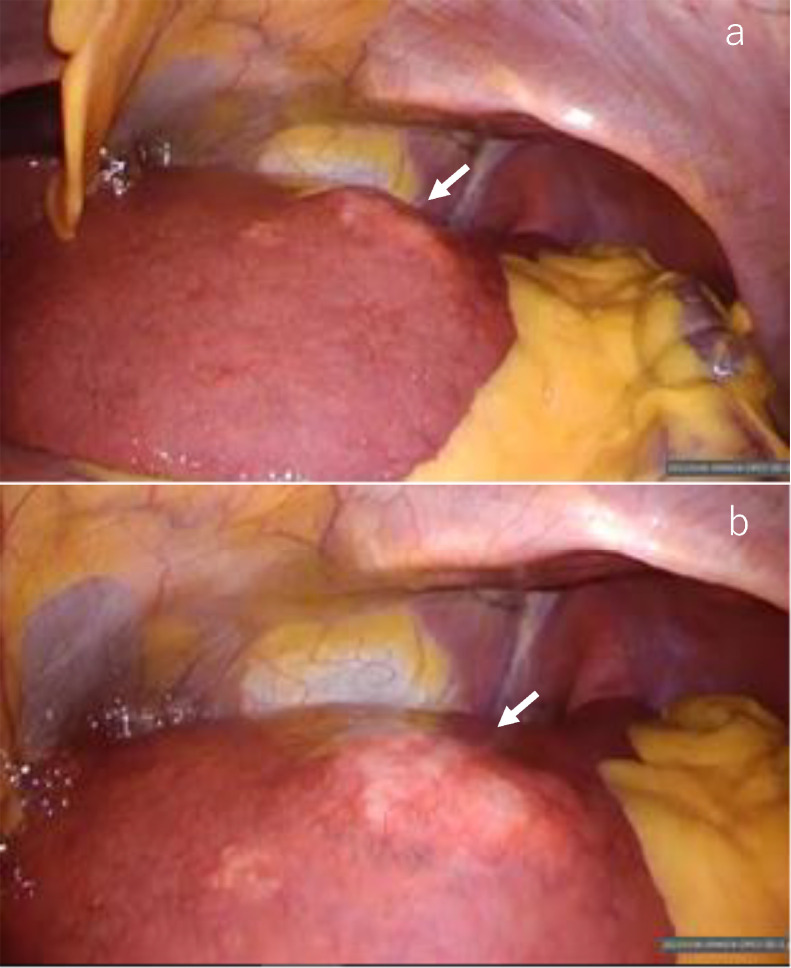
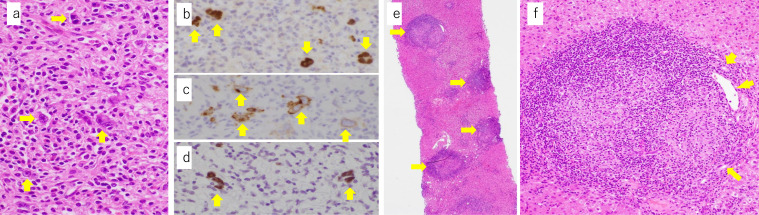
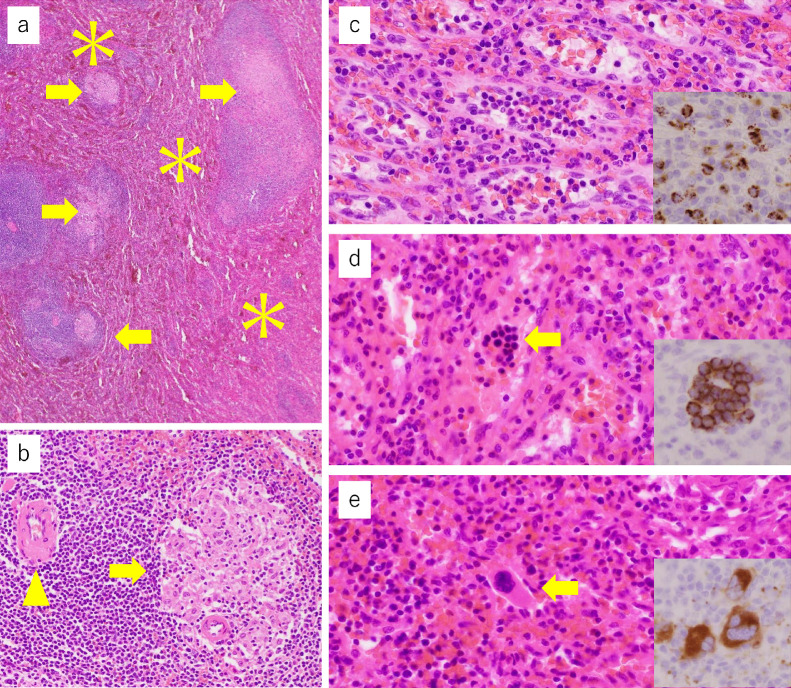
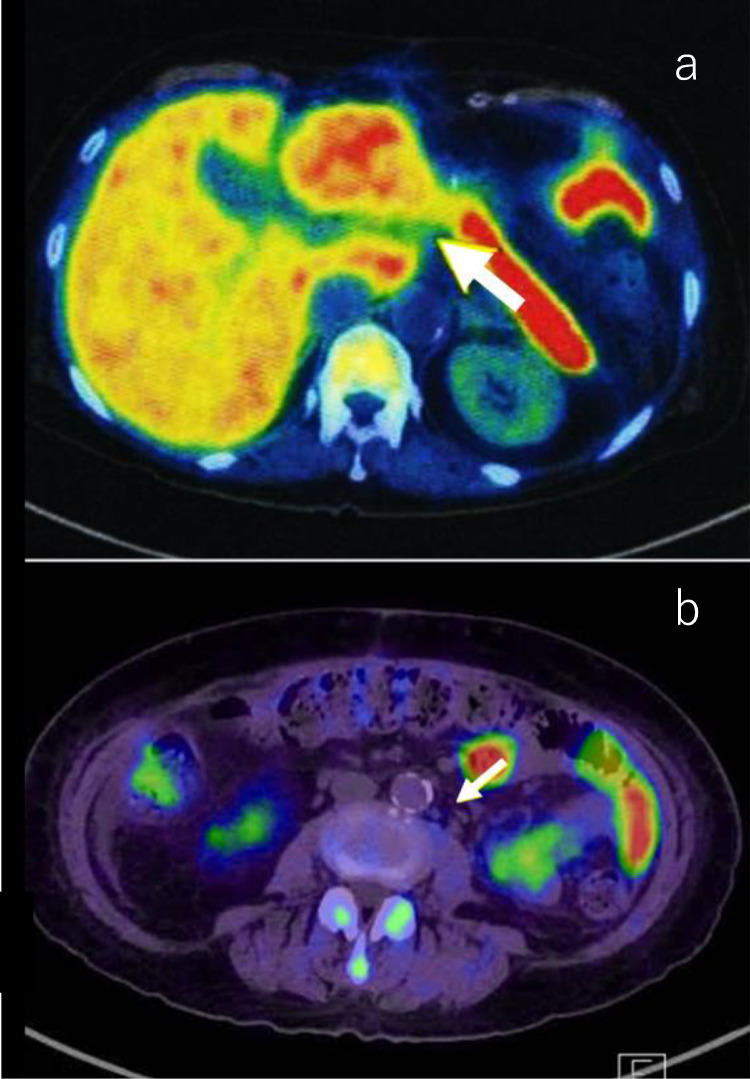
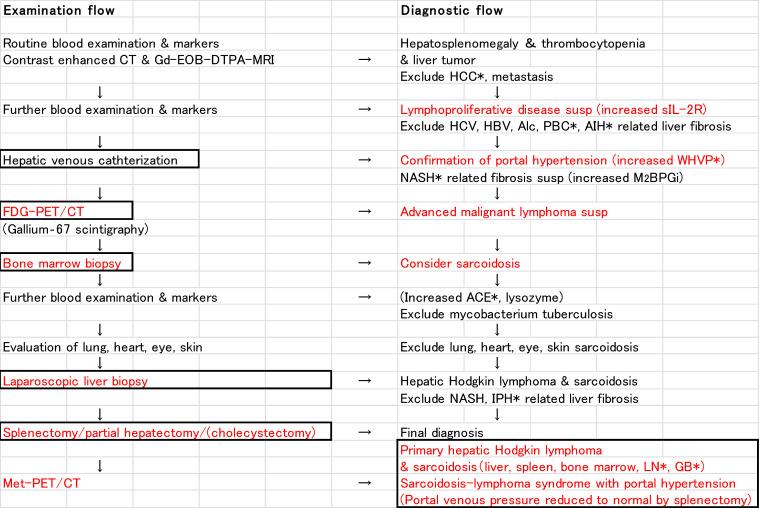
Sarcoidosis-lymphoma syndrome associated with portal hypertension is very rare. A 68-year-old female presented with a 5 kg weight loss in 6 months. Soluble interleukin-2 receptor activity was increased and total platelet count was decreased. Contrast-enhanced computed tomography showed the presence of hepatosplenomegaly and a 3 cm-sized tumor in segment 3 of the liver. The hepatic venous catheterization showed mild portal hypertension. On fluorodeoxyglucose-positron emission tomography/computed tomography, progressive malignant lymphoma was suspected. However, bone marrow biopsy showed multiple noncaseating granulomas. A laparoscopic liver biopsy revealed that the liver tumor had features of Hodgkin lymphoma. There were multiple noncaseating epithelioid granulomas in the portal tracts of the liver. Splenectomy for splenomegaly and partial hepatectomy for the liver tumor were performed. Pathological examination of the resected specimens revealed multiple noncaseating epithelioid granulomas in the liver and spleen. Histopathology of the liver tumor confirmed classic Hodgkin lymphoma with mixed cellularity. We conclude that hepatic venous catheterization, positron emission tomography/computed tomography, and pathological examinations of bone marrow, liver, and spleen are crucial for the diagnosis of sarcoidosis-lymphoma syndrome associated with portal hypertension.
Keywords: Hepatic sarcoidosis; Laparoscopic liver biopsy; PET/CT; Portal hypertension; Primary hepatic Hodgkin lymphoma; Sarcoidosis-lymphoma syndrome.
© 2021 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
