

Partial Nephrectomy Versus Radical Nephrectomy for Clinical T2 or Higher Stage Renal Tumors: A Systematic Review and Meta-Analysis
- PMID: 34178668
- PMCID: PMC8222682
- DOI: 10.3389/fonc.2021.680842
Partial Nephrectomy Versus Radical Nephrectomy for Clinical T2 or Higher Stage Renal Tumors: A Systematic Review and Meta-Analysis
Abstract
Objective: The choice of surgical method for clinically diagnosed T2 or higher stage kidney cancer remains controversial. Here, we systematically reviewed and collected published comparative studies on renal function, oncologic outcomes, and perioperative results of partial nephrectomy (PN) versus radical nephrectomy (RN) for larger renal tumors (T2 and above), and performed a meta-analysis.
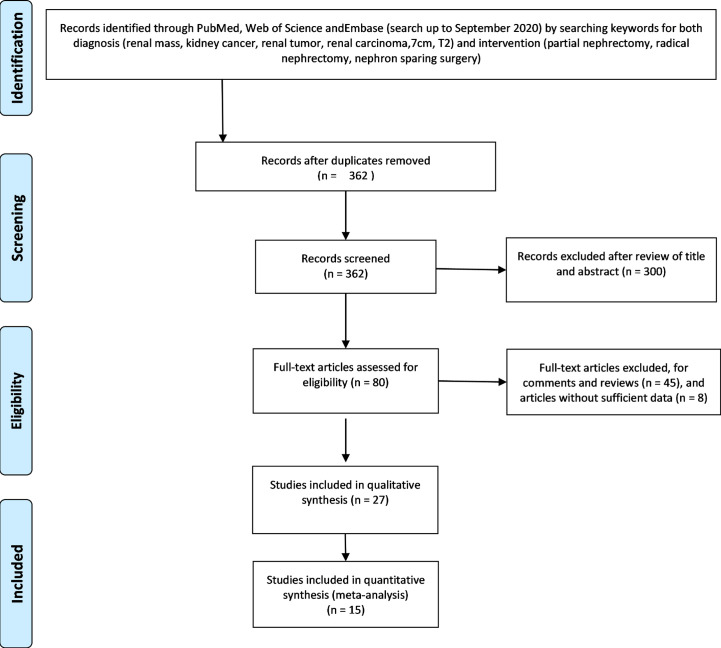
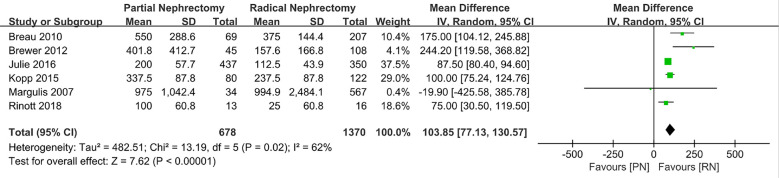
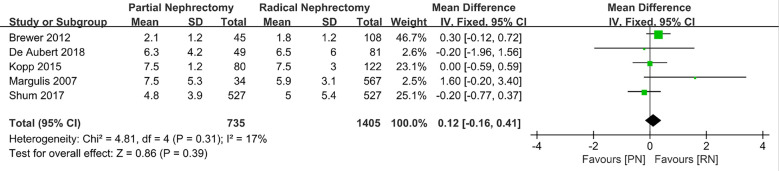
Evidence acquisition: Following searches of PubMed, Web of Science, and Embase, the original studies on PN vs. RN in the treatment of T2 renal cancer were screened through strict inclusion and exclusion criteria. RevMan 5.4 was used for data analysis of the perioperative results, renal function, and oncologic outcomes of the two surgical methods for T2 renal tumor therapy. The weighted mean difference was used as the combined effect size for continuous variables, while the odds ratio (OR) or risk ratio (RR) was used as the combined effect size for binary variables. Both variables used a 95% confidence interval (CI) to estimate statistical accuracy. In cases with low heterogeneity, the fixed-effects model was used to pool the estimated value; otherwise, the random-effects model was used when significant heterogeneity was detected.
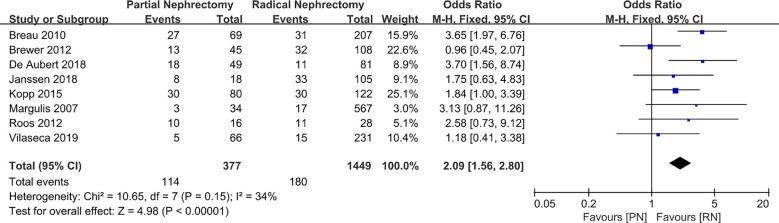
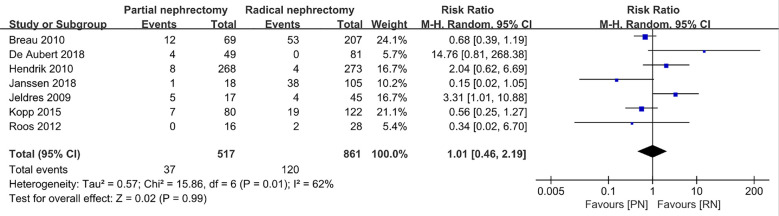
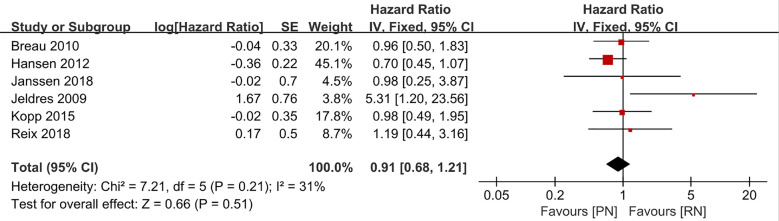
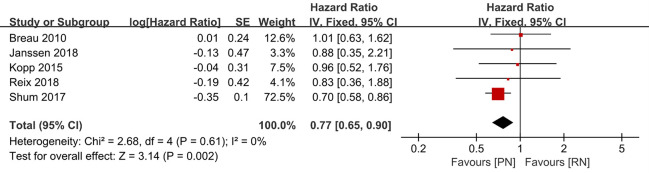
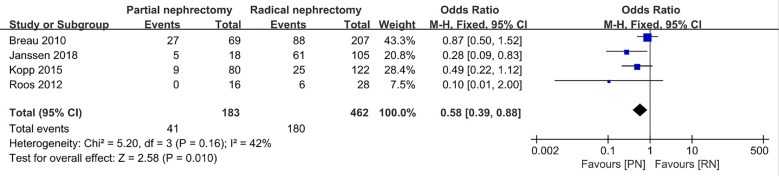
Results: Fifteen retrospective studies including 5,056 patients who underwent nephrectomy (PN: 1975, RN: 3081) were included. The decline in estimated GFR (eGFR) after PN was lower than RN [(MD: -11.74 ml/min/1.73 m2; 95% CI: -13.15, -10.32; p < 0.00001)]. The postoperative complication rate of PN was higher than that of PN (OR: 2.09; 95% CI: 1.56, 2.80; p < 0.00001)], and the postoperative overall survival (OS) of PN was higher than that of RN (HR: 0.77; 95% CI: 0.65, 0.90; p = 0.002), and tumor recurrence (RR, 0.69; 95% CI: 0.53, 0.90; p = 0.007). No obvious publication bias was found in the funnel chart of the OS rates of the two groups of patients.
Conclusions: PN is beneficial for patients with T2 renal tumors in terms of OS and renal function protection. However, it is also associated with a higher risk of surgical complications.
Keywords: kidney cancer; meta-analysis; oncologic outcome; partial nephrectomy; radical nephrectomy; renal function.
Copyright © 2021 Huang, Zhang, Wang and Hu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






Similar articles
-
Partial nephrectomy versus radical nephrectomy for large (≥ 7 cm) renal tumors: A systematic review and meta-analysis.Urol Oncol. 2019 Apr;37(4):263-272. doi: 10.1016/j.urolonc.2018.12.015. Epub 2019 Jan 28. Urol Oncol. 2019. PMID: 30704957
-
Partial nephrectomy versus radical nephrectomy for cT2 or greater renal tumors: a systematic review and meta-analysis.Minerva Urol Nefrol. 2019 Oct;71(5):435-444. doi: 10.23736/S0393-2249.19.03470-2. Epub 2019 Jul 8. Minerva Urol Nefrol. 2019. PMID: 31287256
-
Overall survival and development of stage IV chronic kidney disease in patients undergoing partial and radical nephrectomy for benign renal tumors.Eur Urol. 2013 Oct;64(4):600-6. doi: 10.1016/j.eururo.2012.12.023. Epub 2012 Dec 25. Eur Urol. 2013. PMID: 23280319
-
Partial nephrectomy provides equivalent oncologic outcomes and better renal function preservation than radical nephrectomy for pathological T3a renal cell carcinoma: A meta-analysis.Int Braz J Urol. 2021 Jan-Feb;47(1):46-60. doi: 10.1590/S1677-5538.IBJU.2020.0167. Int Braz J Urol. 2021. PMID: 32271510 Free PMC article. Review.
-
Partial nephrectomy is not associated with an overall survival advantage over radical nephrectomy in elderly patients with stage Ib-II renal masses: An analysis of the national cancer data base.Cancer. 2018 Oct 1;124(19):3839-3848. doi: 10.1002/cncr.31582. Epub 2018 Sep 12. Cancer. 2018. PMID: 30207380
Cited by
-
Partial Nephrectomy for T1b/T2 Renal Mass: An Added Shift from Radical Nephrectomy.J Kidney Cancer VHL. 2022 Oct 6;9(4):1-5. doi: 10.15586/jkcvhl.v9i4.255. eCollection 2022. J Kidney Cancer VHL. 2022. PMID: 36313129 Free PMC article.
-
Differential effects of obesity on perioperative outcomes in renal cell carcinoma patients based on race and ethnicity and neighborhood-level socioeconomic status.Transl Androl Urol. 2024 Apr 30;13(4):548-559. doi: 10.21037/tau-23-421. Epub 2024 Apr 12. Transl Androl Urol. 2024. PMID: 38721286 Free PMC article.
-
Risk factors of recurrence after robot-assisted laparoscopic partial nephrectomy for solitary localized renal cell carcinoma.Sci Rep. 2024 Feb 23;14(1):4481. doi: 10.1038/s41598-023-51070-8. Sci Rep. 2024. PMID: 38396061 Free PMC article.
-
Laser speckle contrast imaging compared with indocyanine green in renal perfusion of a porcine model.Curr Urol. 2023 Jun;17(2):141-145. doi: 10.1097/CU9.0000000000000155. Epub 2022 Sep 28. Curr Urol. 2023. PMID: 37691993 Free PMC article.
-
Comparing oncologic outcomes of partial and radical nephrectomy for T2 renal cell carcinoma: a propensity score matching cohort study and an external multicenter validation.World J Urol. 2025 Mar 12;43(1):166. doi: 10.1007/s00345-025-05561-0. World J Urol. 2025. PMID: 40072570
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous