

Scaling Up the Family Integrated Care Model in a Level IIIC Neonatal Intensive Care Unit: A Systematic Approach to the Methods and Effort Taken for Implementation
- PMID: 34178899
- PMCID: PMC8219911
- DOI: 10.3389/fped.2021.682097
Scaling Up the Family Integrated Care Model in a Level IIIC Neonatal Intensive Care Unit: A Systematic Approach to the Methods and Effort Taken for Implementation
Abstract
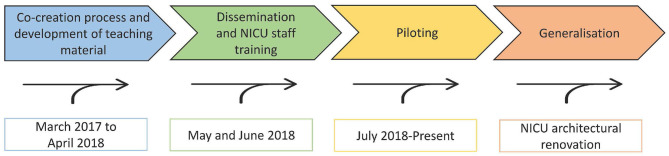
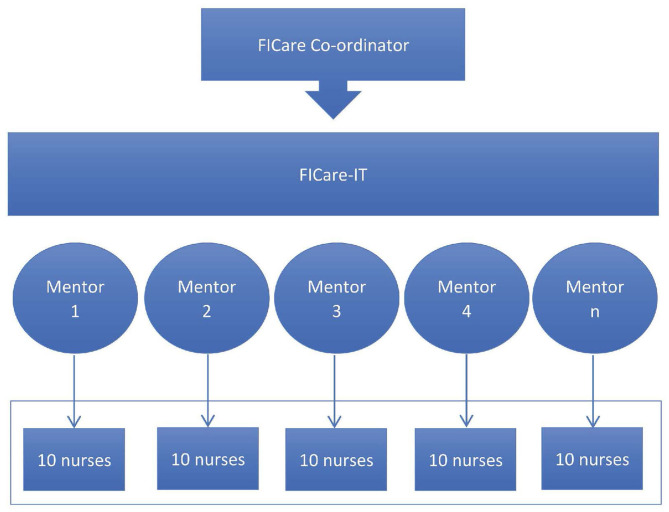
Background: Family Integrated Care (FICare) integrates parents in the direct care of their child while the healthcare personnel act as teachers and guides. To this date, most reports on the feasibility of this model refer to stable preterm infants admitted to Neonatal Intensive Care Units (NICUs). Objectives: To scale up and adapt FICare to make it suitable in level IIIC NICUs, which care for extreme prematurity and other complex medical or surgical neonatal conditions. Materials and Methods: Step 1 was the creation of the FICare implementation team (FICare-IT) and baseline analysis of current procedures for critical care to identify needs, wishes, and requirements; we aimed for protocol elaboration tailored to our cultural, architectural, and clinical context (March 2017 to April 2018). Step 2 as a dissemination strategy by FICare-IT acting as primary trainers and mentors to ensure the education of 90% of nursing staff (May 2018 to July 2018). Step 3 involved piloting and evaluation with the aim to refine the procedure (July 2018 to December 2020). Results: A rigorous but flexible protocol was edited. The FICare educational manual included two curricula: for healthcare professionals/staff (Training the trainers) and for families (Education of caregivers), the latter being categorized in two intervention levels (basic and advanced), depending on the infant care needs and parent's decision. In total, 76 families and 91 infants (74.7% preterm; 18.7% complex surgery; 6.6% others) were enrolled in the pilot. No differences in acceptance rate (overall 86.4%) or in the number of infant-family dyads in the program per month were observed when considering the pre- and post-Covid-19 pandemic periods. All families, except for one who dropped out of the program, completed the agreed individualized training. Mothers spent more time in NICU than fathers (p < 0.05); uninterrupted time spent by mothers in NICU was longer during the pre-pandemic period (p < 0.01). Observed time to reach proficiency by task was within the expected time in 70% of the program contents. The parents revealed educational manuals, workshops, and cot-side teaching sessions as essential for their training, and 100% said they would accept entry into the FICare program again. Conclusions: The principles of the FICare model are suitable for all levels of care in NICUs. Leadership and continuous evaluation/refinement of implementation procedures are essential components to achieve the objectives.
Keywords: FICare; family integrated care; parent education; parent empowerment; parent training.
Copyright © 2021 Moreno-Sanz, Montes, Antón, Serrada, Cabrera and Pellicer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Family Integrated Care (FICare) in Level II Neonatal Intensive Care Units: study protocol for a cluster randomized controlled trial.Trials. 2017 Oct 10;18(1):467. doi: 10.1186/s13063-017-2181-3. Trials. 2017. PMID: 29017578 Free PMC article. Clinical Trial.
-
Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: a multicentre, multinational, cluster-randomised controlled trial.Lancet Child Adolesc Health. 2018 Apr;2(4):245-254. doi: 10.1016/S2352-4642(18)30039-7. Epub 2018 Feb 8. Lancet Child Adolesc Health. 2018. PMID: 30169298 Clinical Trial.
-
Association of a Family Integrated Care Model With Paternal Mental Health Outcomes During Neonatal Hospitalization.JAMA Netw Open. 2022 Jan 4;5(1):e2144720. doi: 10.1001/jamanetworkopen.2021.44720. JAMA Netw Open. 2022. PMID: 35072721 Free PMC article.
-
Family integrated care: State of art and future perspectives.Acta Paediatr. 2025 Apr;114(4):710-730. doi: 10.1111/apa.17272. Epub 2024 May 13. Acta Paediatr. 2025. PMID: 38738866 Review.
-
Family integrated care: Supporting parents as primary caregivers in the neonatal intensive care unit.Pediatr Investig. 2021 Jun 18;5(2):148-154. doi: 10.1002/ped4.12277. eCollection 2021 Jun. Pediatr Investig. 2021. PMID: 34179713 Free PMC article. Review.
Cited by
-
RISEinFAMILY project: the integration of families at neonatal intensive care units (NICUs) to empower them as primary caregivers: study protocol for a stepped wedge cluster controlled trial.Trials. 2024 Apr 10;25(1):248. doi: 10.1186/s13063-024-08043-7. Trials. 2024. PMID: 38594733 Free PMC article.
-
Collaborating to Improve Neonatal Care: ParentAl Participation on the NEonatal Ward-Study Protocol of the neoPARTNER Study.Children (Basel). 2023 Aug 30;10(9):1482. doi: 10.3390/children10091482. Children (Basel). 2023. PMID: 37761442 Free PMC article.
-
Application of Kern's framework to development of a family integrated care curriculum for neonatal intensive care units.Int J Med Educ. 2023 Dec 27;14:197-200. doi: 10.5116/ijme.6566.4b2c. Int J Med Educ. 2023. PMID: 38170949 Free PMC article. No abstract available.
-
Short and mid-term neonatal outcomes in high-risk infants undergoing FICare: a case control study.Pediatr Res. 2025 Jan;97(1):286-292. doi: 10.1038/s41390-024-03307-z. Epub 2024 Jun 10. Pediatr Res. 2025. PMID: 38858503 Free PMC article.
-
Neonatal outcomes from a quasi-experimental clinical trial of Family Integrated Care versus Family-Centered Care for preterm infants in U.S. NICUs.BMC Pediatr. 2022 Nov 22;22(1):674. doi: 10.1186/s12887-022-03732-1. BMC Pediatr. 2022. PMID: 36418988 Free PMC article. Clinical Trial.
References
-
- Melnyk BM, Feinstein NF, Alpert-Gillis L, Fairbanks E, Crean HF, Sinkin RA, et al. . Reducing premature infants' length of stay and improving parents' mental health outcomes with the creating opportunities for parent empowerment (COPE) neonatal intensive care unit program: a randomized, controlled trial. Pediatrics. (2006) 118:e1414–27. 10.1542/peds.2005-2580 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous