

Prospective evaluation of intensity-modulated radiotherapy toxicity in extremity soft tissue sarcomas patients: A role for irradiated healthy soft tissue volume?
- PMID: 34179521
- PMCID: PMC8213831
- DOI: 10.1016/j.ctro.2021.05.007
Prospective evaluation of intensity-modulated radiotherapy toxicity in extremity soft tissue sarcomas patients: A role for irradiated healthy soft tissue volume?
Abstract
Aim: To prospectively assess toxicities of curative-intent intensity-modulated conformal radiotherapy (IMRT) in patients with extremity soft tissue sarcomas (ESTS).
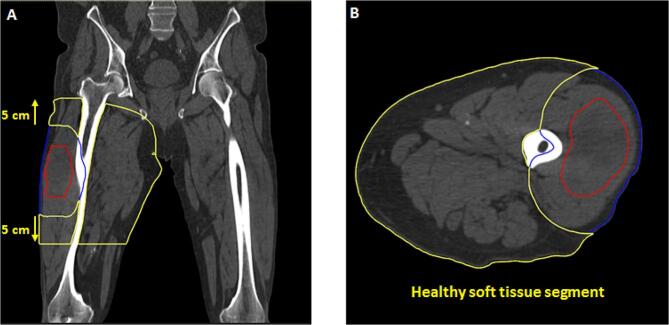
Methods: Data from 59 consecutive patients with ESTS between 2014 and 2019 were both retrospectively and prospectively analysed. Toxicity data were collected both by confidential mailed survey (39% completed) and medical charts, and graded according to CTCAE v5.0. Normal tissues dosimetric data (healthy soft tissue segment, joint and bone) were included. The healthy soft tissue segment was created by adding 5 cm on either side of the PTV on CT axial slices, the PTV and bone (and articulation if present) were then removed from the generated volume.
Results: IMRT was delivered post-operatively for nearly half of patients (n = 24, 41%), preoperatively for 18 (31%) and exclusively for 17 (28%; salvage: 13% or immediately inoperable: 15%). The median total dose delivered to the planned target volume (PTV) was 50.4 Gy (36-68 Gy) and 13 patients (22%) received a boost. With a median follow-up of 27 months (6-94 months), a total of 87 late effects were identified in 44/59 (75%) patients: 89% G1-2, and 11% G3-4. The main G1-2 toxicities were: functional limitation (36%), oedema (29%), gait disorders (20%), neurological disorders (20%) and chronic pain (32%). G3-4 toxicities were pain (n = 2), arterial stricture (n = 1) and a chronic wound requiring skin graft (n = 2). No bone fracture was observed. Quality of life was rated as good or very good in 70% patients who completed the survey. Larger (>3500 cm3) healthy soft tissue segment volume was associated with decreased late toxicities (p = 0.02). No other predictive factor of toxicity was identified. The 2-year rates of local control, overall survival and recurrence-free survival were 90%, 90% and 64%, respectively.
Conclusion: Healthy soft tissue segment volume influenced toxicity. Long-term prospective monitoring in a homogeneous population remains critical to assess the impact of IMRT induced chronic toxicity in ESTS patients. This should ideally lead to a validated normal tissue dose constraint (e.g.: healthy soft tissue segment volume > 3500 cm3) to recommend for practitioners to help reduce the late toxicity risk.
Keywords: Intensity-modulated; Radiotherapy; Sarcomas; Soft tissue neoplasm; Surgery; Toxicity.
© 2021 Published by Elsevier B.V. on behalf of European Society for Radiotherapy and Oncology.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Rosenberg S.A., Tepper J., Glatstein E., Costa J., Baker A., BRENNAM M. The treatment of soft-tissue sarcomas of the extremities: prospective randomized evaluations of (1) limb-sparing surgery plus radiation therapy compared with amputation and (2) the role of adjuvant chemotherapy. Ann Surg. 1982;196(3):305–315. - PMC - PubMed
-
- Pisters P.W., Harrison L.B., Leung D.H., Woodruff J.M., Casper E.S., Brennan M.F. Long-term results of a prospective randomized trial of adjuvant brachytherapy in soft tissue sarcoma. J Clin Oncol Off J Am Soc Clin Oncol. 1996;14(3):859–868. - PubMed
-
- Yang J.C., Chang A.E., Baker A.R., Sindelar W.F., Danforth D.N., Topalian S.L. Randomized prospective study of the benefit of adjuvant radiation therapy in the treatment of soft tissue sarcomas of the extremity. J Clin Oncol Off J Am Soc Clin Oncol. 1998;16(1):197–203. - PubMed
-
- O'Sullivan B., Davis A.M., Turcotte R., Bell R., Catton C., Chabot P. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial. Lancet. 2002;359(9325):2235–2241. - PubMed
-
- Levy A., Bonvalot S., Bellefqih S., Terrier P., Le Cesne A., Le Péchoux C. Is dose de-escalation possible in sarcoma patients treated with enlarged limb sparing resection? Radiother Oncol. 2018;126(3):493–498. - PubMed
LinkOut - more resources
Full Text Sources
