

Endovascular Stent-Graft Repair of the Ascending Aorta: Assessment of a Specific Novel Stent-Graft Design in Phantom, Cadaveric, and Clinical Application
- PMID: 34180002
- PMCID: PMC8382630
- DOI: 10.1007/s00270-021-02859-5
Endovascular Stent-Graft Repair of the Ascending Aorta: Assessment of a Specific Novel Stent-Graft Design in Phantom, Cadaveric, and Clinical Application
Abstract
Purpose: To test a stent-graft specifically designed for the ascending aorta in phantom, cadaver, and clinical application, and to measure deployment accuracy to overcome limitations of existing devices.
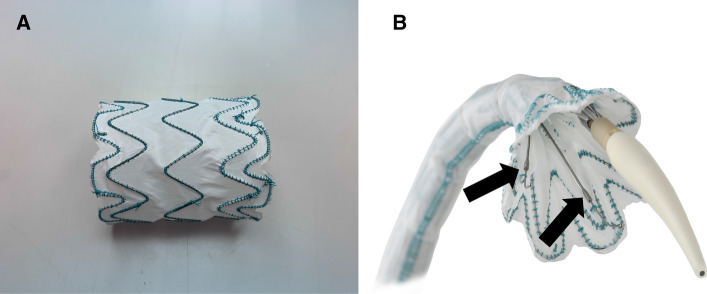
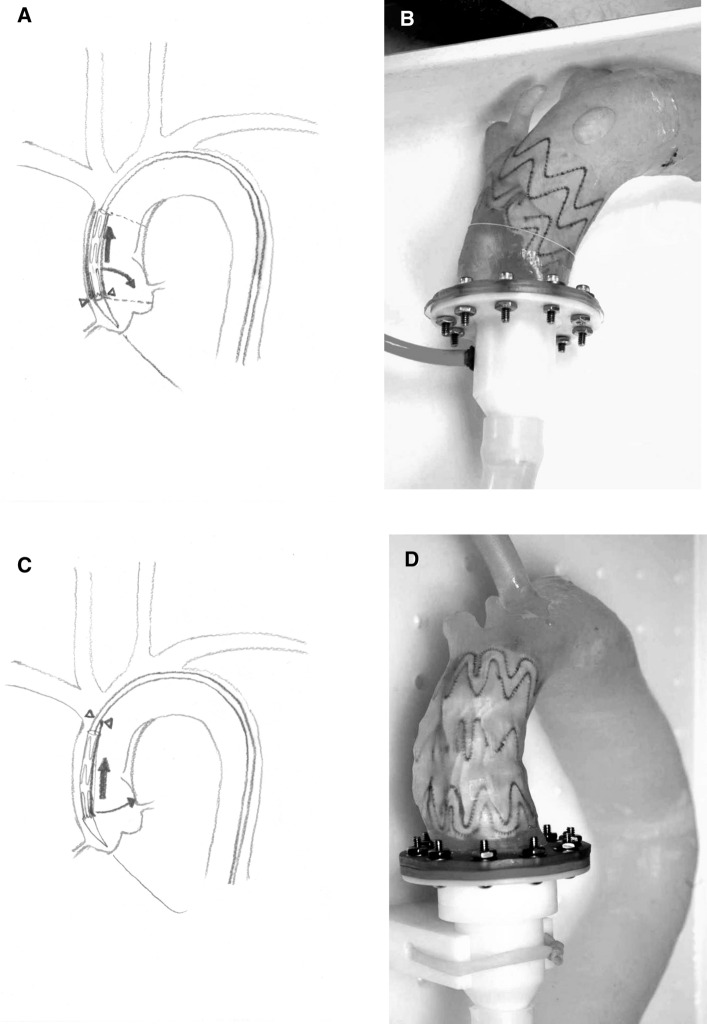
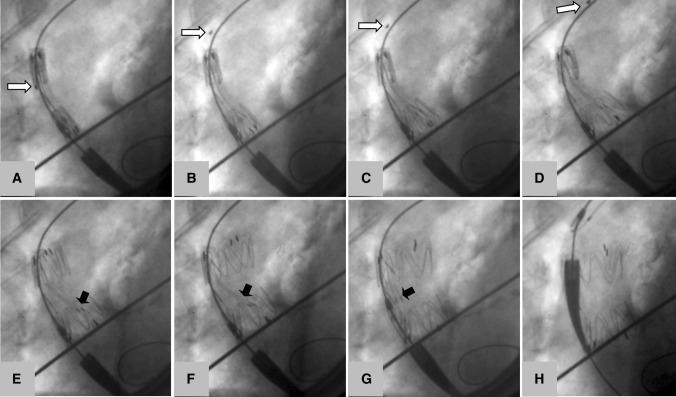
Methods: A stent-graft has been designed with support wires to fixate the apices toward the inner curvature, thereby eliminating the forward movement of the proximal end which can happen with circumferential tip capture systems. The device was deployed in three aortic phantoms, and in four cadavers, deployment precision was measured. Subsequently, the device was implanted in a patient to exclude a pseudoaneurysm originating from the distal anastomosis after ascending aortic replacement.
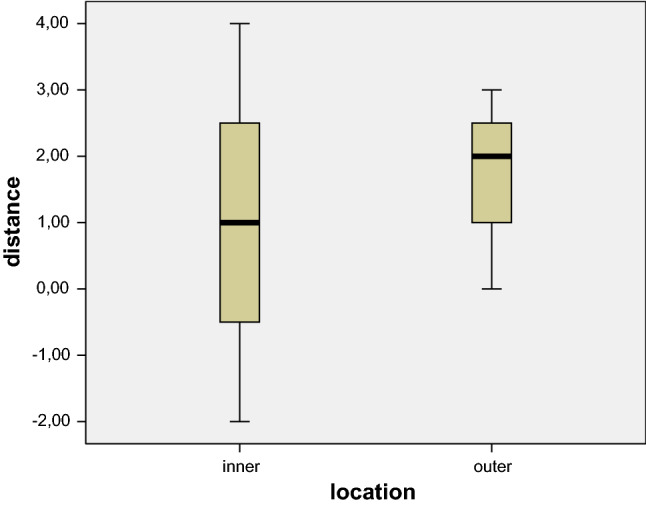
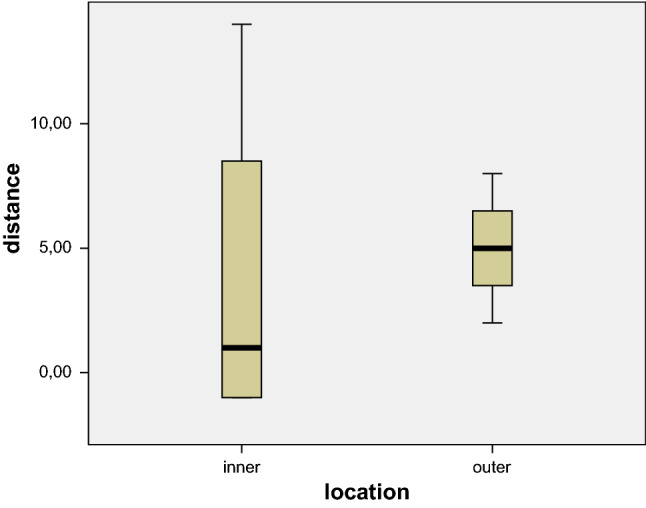
Results: The stent-grafts were successfully deployed in all phantoms and cadavers. Deployment accuracy of the proximal end of the stent-graft was within 1 mm proximally and 14 mm distally to the intended landing zone on the inner curvature, and 2-8 mm distal to the intended landing zone on the outer curvature. In clinical application, the pseudoaneurysm could be successfully excluded without complications.
Conclusion: The novel stent-graft design promises accurate placement in the ascending aorta. The differential deployment of the apices at the inner and outer curvatures allows deployment perpendicular to the aortic axis.
Level of evidence: No level of evidence.
Keywords: Ascending TEVAR; Ascending aortic stent-graft; Custom-made stentgraft.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Czerny M, Zimpfer D, Rodler S, Funovics M, Dorfmeister M, Schoder M, Marta G, Weigang E, Gottardi R, Lammer J, Wolner E, Grimm M. Endovascular stent-graft placement of aneurysms involving the descending aorta originating from chronic type B dissections. Ann Thorac Surg. 2007;83(5):1635–1639. doi: 10.1016/j.athoracsur.2006.12.041. - DOI - PubMed
-
- Schoder M, Czerny M, Cejna M, Rand T, Stadler A, Sodeck GH, Gottardi R, Loewe C, Lammer J. Endovascular repair of acute type B aortic dissection: long-term follow-up of true and false lumen diameter changes. Ann Thorac Surg. 2007;83(3):1059–1066. doi: 10.1016/j.athoracsur.2006.10.064. - DOI - PubMed
-
- Gottardi R, Zimpfer D, Funovics M, Schoder M, Lammer J, Wolner E, Czerny M, Grimm M. Mid-term results after endovascular stent-graft placement due to penetrating atherosclerotic ulcers of the thoracic aorta. Eur J Cardiothorac Surg. 2008;33(6):1019–1024. doi: 10.1016/j.ejcts.2007.12.054. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
