

Combined Metabolic Activators Accelerates Recovery in Mild-to-Moderate COVID-19
- PMID: 34180141
- PMCID: PMC8420376
- DOI: 10.1002/advs.202101222
Combined Metabolic Activators Accelerates Recovery in Mild-to-Moderate COVID-19
Abstract
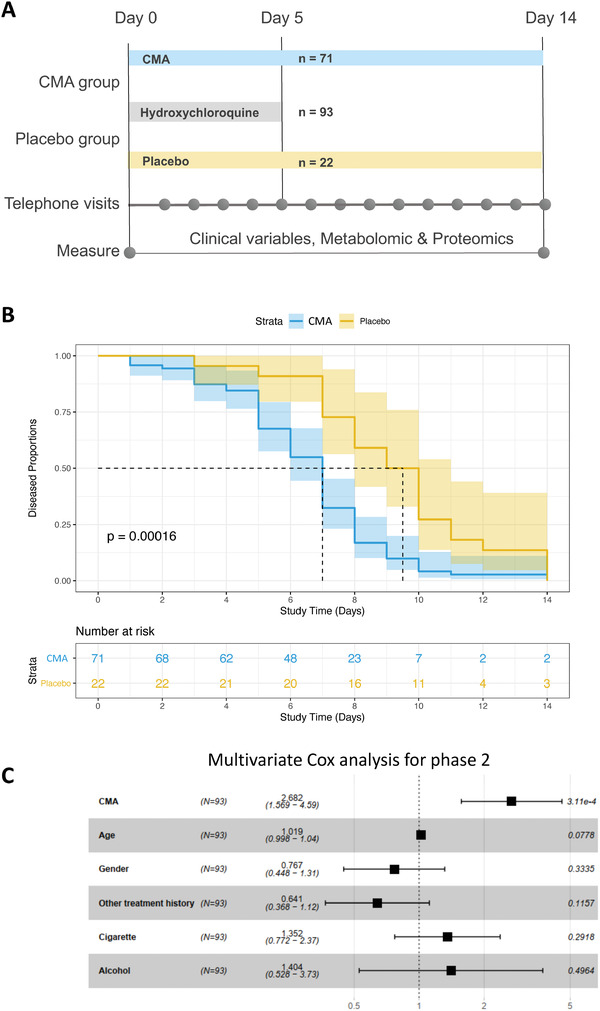
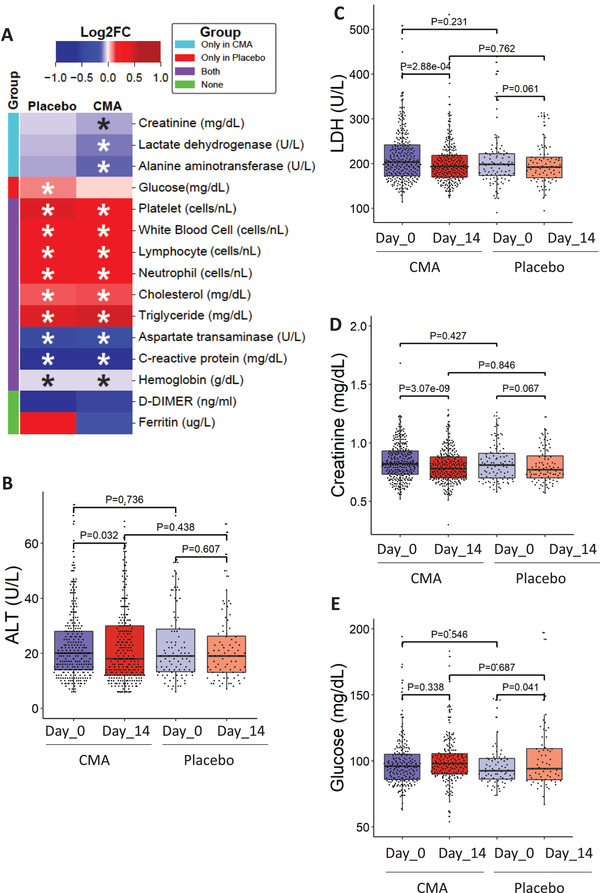
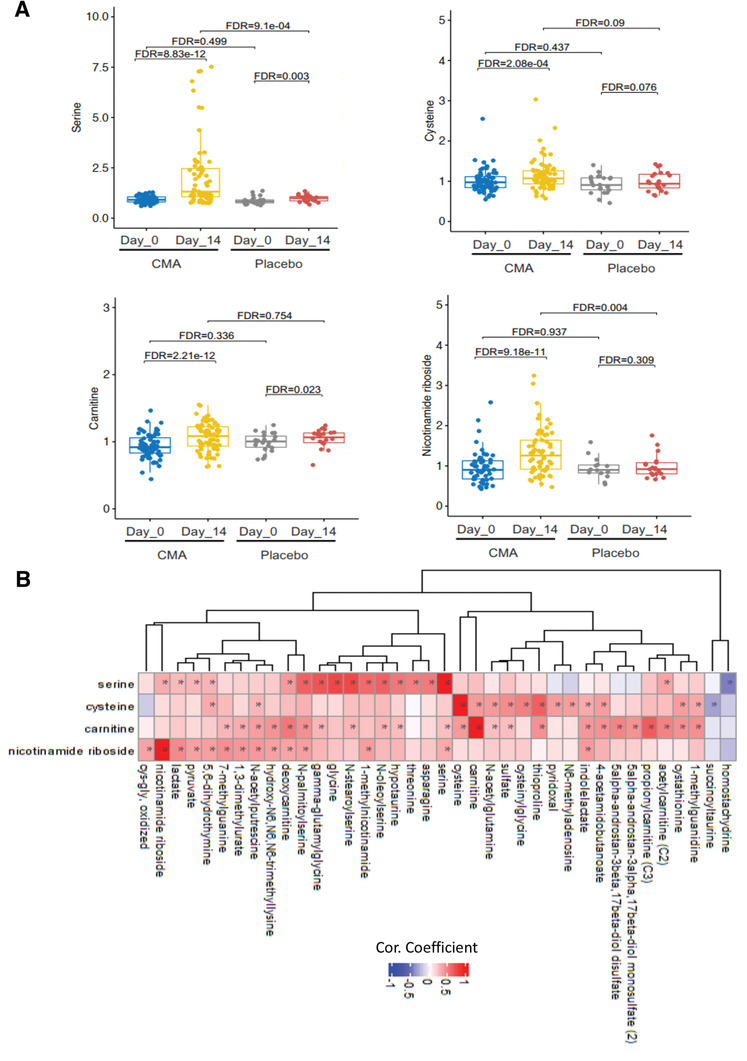
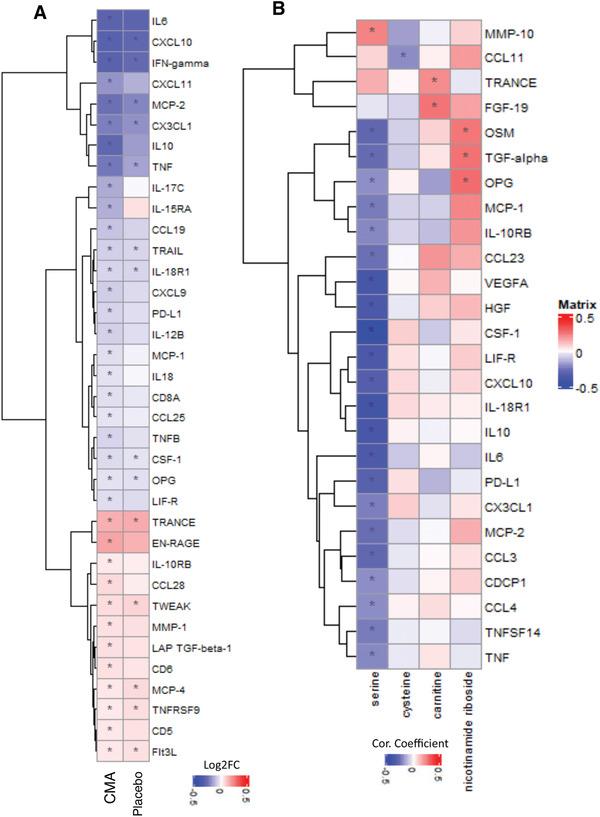
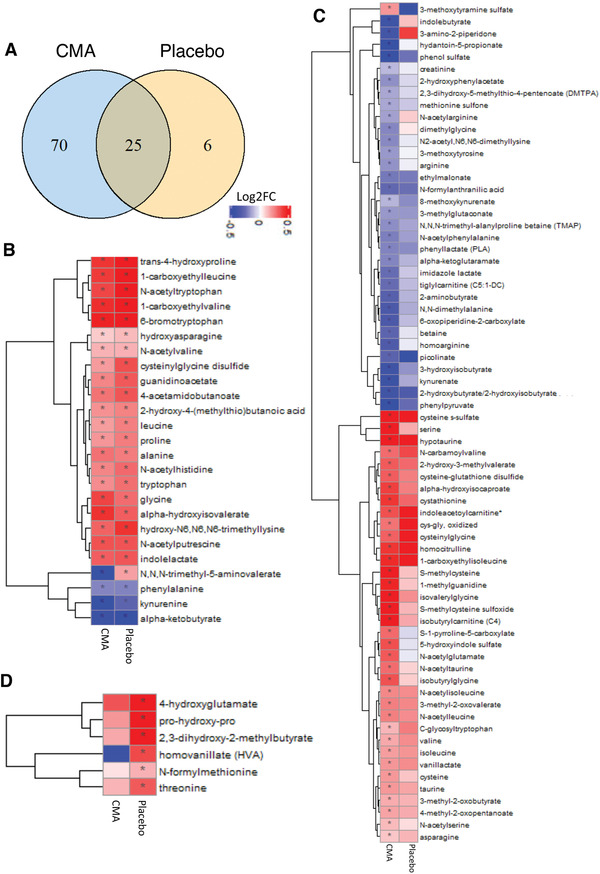
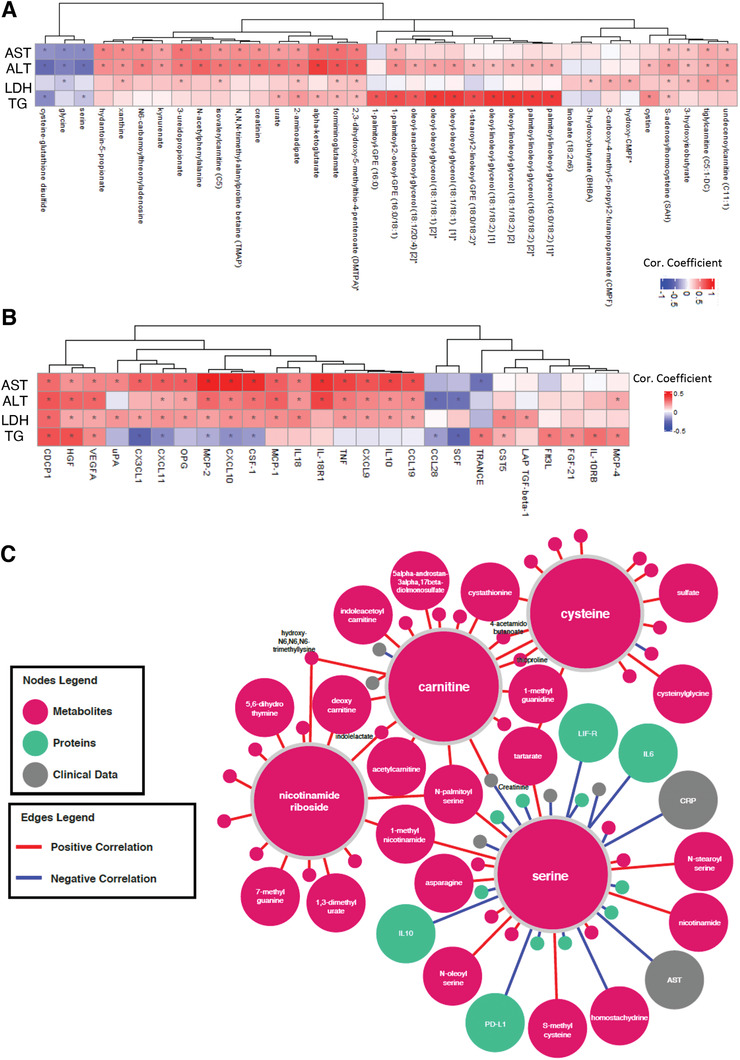
COVID-19 is associated with mitochondrial dysfunction and metabolic abnormalities, including the deficiencies in nicotinamide adenine dinucleotide (NAD+ ) and glutathione metabolism. Here it is investigated if administration of a mixture of combined metabolic activators (CMAs) consisting of glutathione and NAD+ precursors can restore metabolic function and thus aid the recovery of COVID-19 patients. CMAs include l-serine, N-acetyl-l-cysteine, nicotinamide riboside, and l-carnitine tartrate, salt form of l-carnitine. Placebo-controlled, open-label phase 2 study and double-blinded phase 3 clinical trials are conducted to investigate the time of symptom-free recovery on ambulatory patients using CMAs. The results of both studies show that the time to complete recovery is significantly shorter in the CMA group (6.6 vs 9.3 d) in phase 2 and (5.7 vs 9.2 d) in phase 3 trials compared to placebo group. A comprehensive analysis of the plasma metabolome and proteome reveals major metabolic changes. Plasma levels of proteins and metabolites associated with inflammation and antioxidant metabolism are significantly improved in patients treated with CMAs as compared to placebo. The results show that treating patients infected with COVID-19 with CMAs lead to a more rapid symptom-free recovery, suggesting a role for such a therapeutic regime in the treatment of infections leading to respiratory problems.
Keywords: COVID-19; combined metabolic activators; metabolomics; omics data; proteomics.
© 2021 The Authors. Advanced Science published by Wiley-VCH GmbH.
Conflict of interest statement
A.M., J.B., and M.U. are the founders and shareholders of ScandiBio Therapeutics and they filed a patent application on the use of CMA to treat COVID‐19 patients. The other authors declare no competing interests.
Figures

References
-
- Gupta A., Madhavan M. V., Sehgal K., Nair N., Mahajan S., Sehrawat T. S., Bikdeli B., Ahluwalia N., Ausiello J. C., Wan E. Y., Freedberg D. E., Kirtane A. J., Parikh S. A., Maurer M. S., Nordvig A. S., Accili D., Bathon J. M., Mohan S., Bauer K. A., Leon M. B., Krumholz H. M., Uriel N., Mehra M. R., Elkind M. S. V., Stone G. W., Schwartz A., Ho D. D., Bilezikian J. P., Landry D. W., Nat. Med. 2020, 26, 1017. - PMC - PubMed
-
- Johns Hopkins University of Medicine (2021 January 11).
-
- Zhu L., She Z.‐G., Cheng X., Qin J.‐J., Zhang X.‐J., Cai J., Lei F., Wang H., Xie J., Wang W., Li H., Zhang P., Song X., Chen X., Xiang M., Zhang C., Bai L., Xiang D., Chen M.‐M., Liu Y., Yan Y., Liu M., Mao W., Zou J., Liu L., Chen G., Luo P., Xiao B., Zhang C., Zhang Z., Lu Z., Wang J., Lu H., Xia X., Wang D., Liao X., Peng G., Ye P., Yang J., Yuan Y., Huang X., Guo J., Zhang B.‐H., Li H., Cell Metab. 2020, 31, 1068. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical