

Comparative Effectiveness of Sodium-Glucose Cotransporter 2 Inhibitors vs Sulfonylureas in Patients With Type 2 Diabetes
- PMID: 34180939
- PMCID: PMC8240007
- DOI: 10.1001/jamainternmed.2021.2488
Comparative Effectiveness of Sodium-Glucose Cotransporter 2 Inhibitors vs Sulfonylureas in Patients With Type 2 Diabetes
Erratum in
-
Errors in Figure 2 and eTable 3 in the Supplement.JAMA Intern Med. 2021 Nov 1;181(11):1544. doi: 10.1001/jamainternmed.2021.5417. JAMA Intern Med. 2021. PMID: 34515739 Free PMC article. No abstract available.
Abstract
Importance: In the treatment of type 2 diabetes, evidence of the comparative effectiveness of sodium-glucose cotransporter 2 (SGLT2) inhibitors vs sulfonylureas-the second most widely used antihyperglycemic class after metformin-is lacking.
Objective: To evaluate the comparative effectiveness of SGLT2 inhibitors and sulfonylureas associated with the risk of all-cause mortality among patients with type 2 diabetes using metformin.
Design, setting, and participants: A cohort study used data from the US Department of Veterans Affairs compared the use of SGLT2 inhibitors vs sulfonylureas in individuals receiving metformin for treatment of type 2 diabetes. A total of 23 870 individuals with new use of SGLT2 inhibitors and 104 423 individuals with new use of sulfonylureas were enrolled between October 1, 2016, and February 29, 2020, and followed up until January 31, 2021.
Exposures: New use of SGLT2 inhibitors or sulfonylureas.
Main outcomes and measures: This study examined the outcome of all-cause mortality. Predefined variables and covariates identified by a high-dimensional variable selection algorithm were used to build propensity scores. The overlap weighting method based on the propensity scores was used to estimate the intention-to-treat effect sizes of SGLT2 inhibitor compared with sulfonylurea therapy. The inverse probability of the treatment adherence weighting method was used to estimate the per-protocol effect sizes.
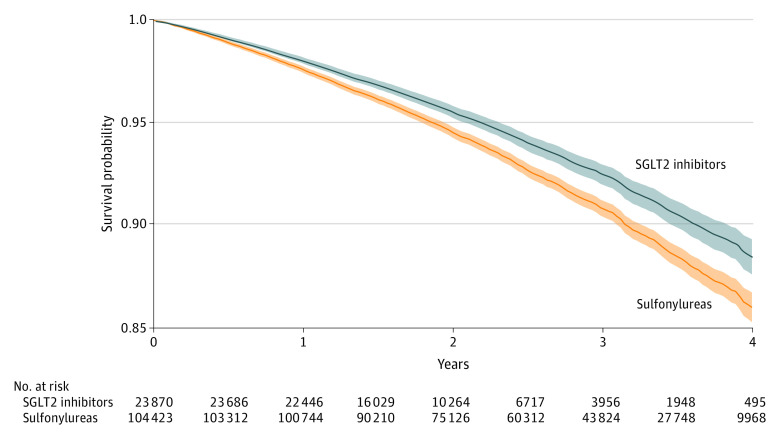
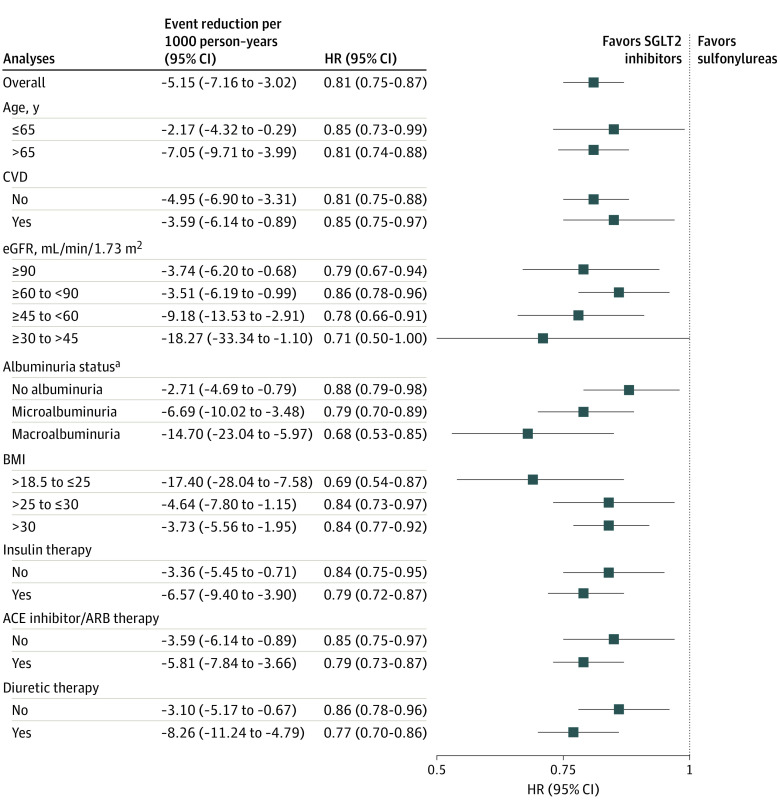
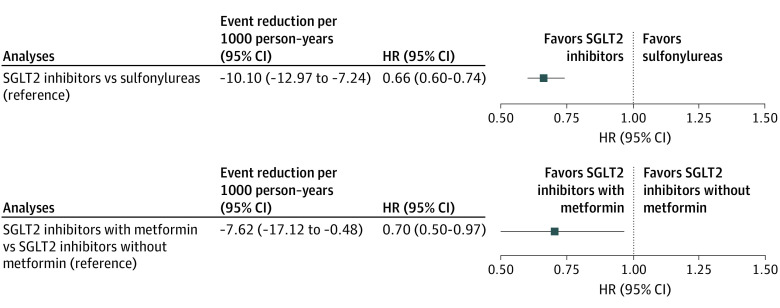
Results: Among the 128 293 participants (mean [SD] age, 64.60 [9.84] years; 122 096 [95.17%] men), 23 870 received an SGLT2 inhibitor and 104 423 received a sulfonylurea. Compared with sulfonylureas, SGLT2 inhibitors were associated with reduced risk of all-cause mortality (hazard ratio [HR], 0.81; 95% CI, 0.75-0.87), yielding an event rate difference of -5.15 (95% CI, -7.16 to -3.02) deaths per 1000 person-years. Compared with sulfonylureas, SGLT2 inhibitors were associated with a reduced risk of death, regardless of cardiovascular disease status, in several categories of estimated glomerular filtration rate (including rates from >90 to ≤30 mL/min/1.73 m2) and in participants with no albuminuria (albumin to creatinine ratio [ACR] ≤30 mg/g), microalbuminuria (ACR >30 to ≤300 mg/g), and macroalbuminuria (ACR >300 mg/g). In per-protocol analyses, continued use of SGLT2 inhibitors was associated with a reduced risk of death compared with continued use of sulfonylureas (HR, 0.66; 95% CI, 0.60-0.74; event rate difference, -10.10; 95% CI, -12.97 to -7.24 deaths per 1000 person-years). In additional per-protocol analyses, continued use of SGLT2 inhibitors with metformin was associated with a reduced risk of death compared with SGLT2 inhibitor treatment without metformin (HR, 0.70; 95% CI, 0.50-0.97; event rate difference, -7.62; 95% CI, -17.12 to -0.48 deaths per 1000 person-years).
Conclusions and relevance: In this comparative effectiveness study analyzing data from the US Department of Veterans Affairs, among patients with type 2 diabetes receiving metformin therapy, SGLT2 inhibitor treatment was associated with a reduced risk of all-cause mortality compared with sulfonylureas. The results provide data from a real-world setting that might help guide the choice of antihyperglycemic therapy.
Conflict of interest statement
Figures
Comment in
-
Sodium-Glucose Cotransporter 2 Inhibitors vs Sulfonylureas: The Price of Prevention.JAMA Intern Med. 2021 Aug 1;181(8):1054. doi: 10.1001/jamainternmed.2021.2487. JAMA Intern Med. 2021. PMID: 34180948 No abstract available.
-
Comparative Effectiveness of Sodium-Glucose Cotransporter 2 Inhibitors vs Sulfonylureas in Patients With Type 2 Diabetes-Reply.JAMA Intern Med. 2022 Jan 1;182(1):93-94. doi: 10.1001/jamainternmed.2021.6334. JAMA Intern Med. 2022. PMID: 34724023 No abstract available.
-
Comparative Effectiveness of Sodium-Glucose Cotransporter 2 Inhibitors vs Sulfonylureas in Patients With Type 2 Diabetes.JAMA Intern Med. 2022 Jan 1;182(1):93. doi: 10.1001/jamainternmed.2021.6321. JAMA Intern Med. 2022. PMID: 34724024 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
