

Use of intravenous iron and risk of anaphylaxis: A multinational observational post-authorisation safety study in Europe
- PMID: 34181291
- PMCID: PMC8457074
- DOI: 10.1002/pds.5319
Use of intravenous iron and risk of anaphylaxis: A multinational observational post-authorisation safety study in Europe
Abstract
Purpose: This post-authorisation safety study estimated the risk of anaphylaxis in patients receiving intravenous (IV) iron in Europe, with interest in iron dextran and iron non-dextrans. Studies conducted in the United States have reported risk of anaphylaxis to IV iron ranging from 2.0 to 6.8 per 10 000 first treatments.
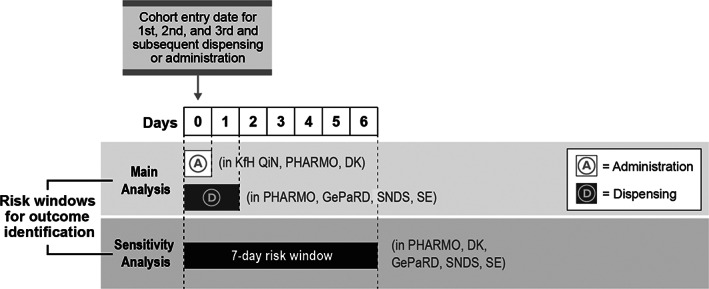
Methods: Cohort study of IV iron new users, captured mostly through pharmacy ambulatory dispensing, from populations covered by health and administrative data sources in five European countries from 1999 to 2017. Anaphylaxis events were identified through an algorithm that used parenteral penicillin as a positive control.
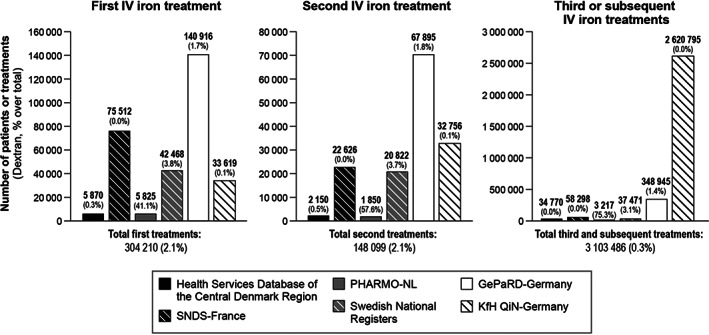
Results: A total of 304 210 patients with a first IV iron treatment (6367 iron dextran), among whom 13-16 anaphylaxis cases were identified and reported as a range to comply with data protection regulations. The pooled unadjusted incidence proportion (IP) ranged from 0.4 (95% confidence interval [CI], 0.2-0.9) to 0.5 (95% CI, 0.3-1.0) per 10 000 first treatments. No events were identified at first dextran treatments. There were 231 294 first penicillin treatments with 30 potential cases of anaphylaxis (IP = 1.2; 95% CI, 0.8-1.7 per 10 000 treatments).
Conclusion: We found an IP of anaphylaxis from 0.4 to 0.5 per 10 000 first IV iron treatments. The study captured only a fraction of IV iron treatments administered in hospitals, where most first treatments are likely to happen. Due to this limitation, the study could not exclude a differential risk of anaphylaxis between iron dextran and iron non-dextrans. The IP of anaphylaxis in users of penicillin was consistent with incidences reported in the literature.
Keywords: IV iron; anaphylaxis; cohort study; dextran; multidatabase; severe hypersensitivity reactions.
© 2021 Vifor (International) AG. Pharmacoepidemiology and Drug Safety published by John Wiley & Sons Ltd.
Conflict of interest statement
The study was funded by a consortium of IV iron marketing authorisation holders and was conducted under a contract including the ENCePP Seal granting the research team independent publication rights.
Figures


References
-
- Auerbach M, Ballard H. Clinical use of intravenous iron: administration, efficacy, and safety. Hematology Am Soc Hematol Educ Program. 2010;2010:338‐347. - PubMed
-
- Bailie GR, Verhoef JJ. Differences in the reporting rates of serious allergic adverse events from intravenous iron by country and population. Clin Adv Hematol Oncol. 2012. Feb;10(2):101‐108. - PubMed
-
- Walsh K, Andrade S, Cocoros N, et al. Sentinel assessment report: parenteral iron and anaphylactoid reactions. US Food and Drug Administration; 22 July 2016. https://www.sentinelinitiative.org/sites/default/files/surveillance‐tool.... Accessed 6 October 2020.
-
- Wang C, Graham DJ, Kane RC, et al. Comparative risk of anaphylactic reactions associated with intravenous iron products. JAMA. 2015;314(19):2062‐2068. - PubMed
-
- Chertow GM, Mason PD, Vaage‐Nilsen O, Ahlmen J. On the relative safety of parenteral iron formulations. Nephrol Dial Transplant. 2004;19(6):1571‐1575. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
