

Direct maternal morbidity and the risk of pregnancy-related deaths, stillbirths, and neonatal deaths in South Asia and sub-Saharan Africa: A population-based prospective cohort study in 8 countries
- PMID: 34181649
- PMCID: PMC8277068
- DOI: 10.1371/journal.pmed.1003644
Direct maternal morbidity and the risk of pregnancy-related deaths, stillbirths, and neonatal deaths in South Asia and sub-Saharan Africa: A population-based prospective cohort study in 8 countries
Abstract
Background: Maternal morbidity occurs several times more frequently than mortality, yet data on morbidity burden and its effect on maternal, foetal, and newborn outcomes are limited in low- and middle-income countries. We aimed to generate prospective, reliable population-based data on the burden of major direct maternal morbidities in the antenatal, intrapartum, and postnatal periods and its association with maternal, foetal, and neonatal death in South Asia and sub-Saharan Africa.
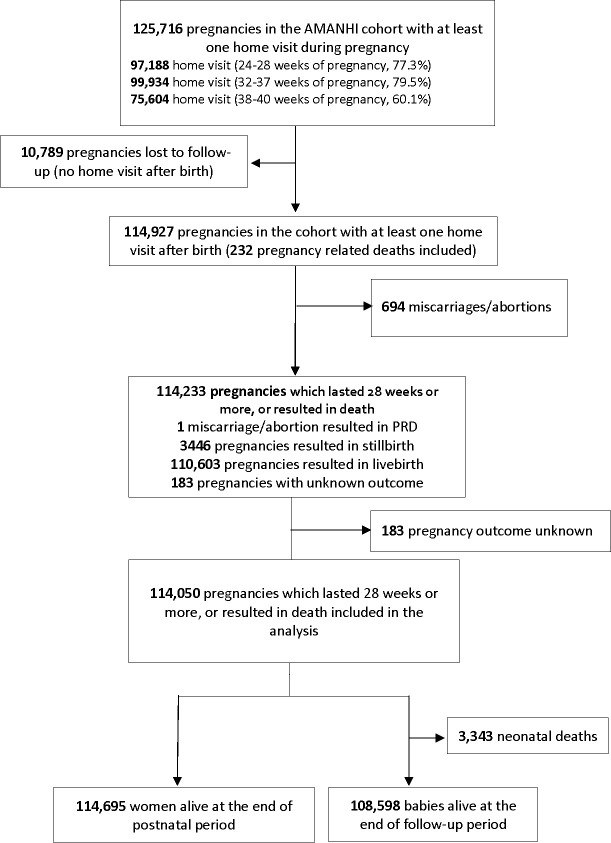
Methods and findings: This is a prospective cohort study, conducted in 9 research sites in 8 countries of South Asia and sub-Saharan Africa. We conducted population-based surveillance of women of reproductive age (15 to 49 years) to identify pregnancies. Pregnant women who gave consent were include in the study and followed up to birth and 42 days postpartum from 2012 to 2015. We used standard operating procedures, data collection tools, and training to harmonise study implementation across sites. Three home visits during pregnancy and 2 home visits after birth were conducted to collect maternal morbidity information and maternal, foetal, and newborn outcomes. We measured blood pressure and proteinuria to define hypertensive disorders of pregnancy and woman's self-report to identify obstetric haemorrhage, pregnancy-related infection, and prolonged or obstructed labour. Enrolled women whose pregnancy lasted at least 28 weeks or those who died during pregnancy were included in the analysis. We used meta-analysis to combine site-specific estimates of burden, and regression analysis combining all data from all sites to examine associations between the maternal morbidities and adverse outcomes. Among approximately 735,000 women of reproductive age in the study population, and 133,238 pregnancies during the study period, only 1.6% refused consent. Of these, 114,927 pregnancies had morbidity data collected at least once in both antenatal and in postnatal period, and 114,050 of them were included in the analysis. Overall, 32.7% of included pregnancies had at least one major direct maternal morbidity; South Asia had almost double the burden compared to sub-Saharan Africa (43.9%, 95% CI 27.8% to 60.0% in South Asia; 23.7%, 95% CI 19.8% to 27.6% in sub-Saharan Africa). Antepartum haemorrhage was reported in 2.2% (95% CI 1.5% to 2.9%) pregnancies and severe postpartum in 1.7% (95% CI 1.2% to 2.2%) pregnancies. Preeclampsia or eclampsia was reported in 1.4% (95% CI 0.9% to 2.0%) pregnancies, and gestational hypertension alone was reported in 7.4% (95% CI 4.6% to 10.1%) pregnancies. Prolonged or obstructed labour was reported in about 11.1% (95% CI 5.4% to 16.8%) pregnancies. Clinical features of late third trimester antepartum infection were present in 9.1% (95% CI 5.6% to 12.6%) pregnancies and those of postpartum infection in 8.6% (95% CI 4.4% to 12.8%) pregnancies. There were 187 pregnancy-related deaths per 100,000 births, 27 stillbirths per 1,000 births, and 28 neonatal deaths per 1,000 live births with variation by country and region. Direct maternal morbidities were associated with each of these outcomes.
Conclusions: Our findings imply that health programmes in sub-Saharan Africa and South Asia must intensify their efforts to identify and treat maternal morbidities, which affected about one-third of all pregnancies and to prevent associated maternal and neonatal deaths and stillbirths.
Trial registration: The study is not a clinical trial.
Conflict of interest statement
We have read the journal’s policy and the authors of this manuscript have the following competing interests: ZAB is a member of the Editorial Board of PLOS Medicine. Remaining authors declared no competing interests.
Figures
References
-
- Alkema L, Chou D, Hogan D, Zhang S, Moller AB, Gemmill A, et al.; United Nations Maternal Mortality Estimation Inter to Agency Group collaborators and technical advisory group. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario to based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter to Agency Group. Lancet. 2016. Jan 30;387(10017):462–74. doi: 10.1016/S0140-6736(15)00838-7 Epub 2015 Nov 13. - DOI - PMC - PubMed
-
- World Health Organization. Why do so many women still die in pregnancy or childbirth? Available from: http://www. who.int/features/qa/12/en/. Accessed: 26 March 2015.
-
- Murray C, Lopez A, editors. Health Dimensions of Sex and Reproduction. Boston: Boston: Harvard University Press; 1998.
-
- Pacagnella RC, Cecatti JG, Camargo RP, Silveira C, Zanardi DT, Souza JP, et al. Rationale for a long–term evaluation of the consequences of potentially life–threatening maternal conditions and maternal “near–miss” incidents using a multidimensional approach. J Obstet Gynaecol Can. 2010;32:730–8. Medline:21050503 doi: 10.1016/s1701-2163(16)34612-6 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
