

Osteoid Osteoma: An Updated Review of Epidemiology, Pathogenesis, Clinical Presentation, Radiological Features, and Treatment Option
- PMID: 34182465
- PMCID: PMC8286494
- DOI: 10.21873/invivo.12459
Osteoid Osteoma: An Updated Review of Epidemiology, Pathogenesis, Clinical Presentation, Radiological Features, and Treatment Option
Abstract
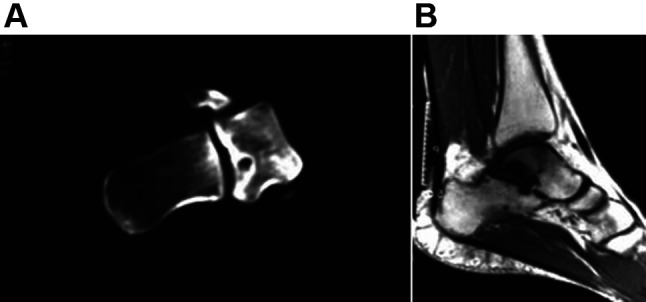
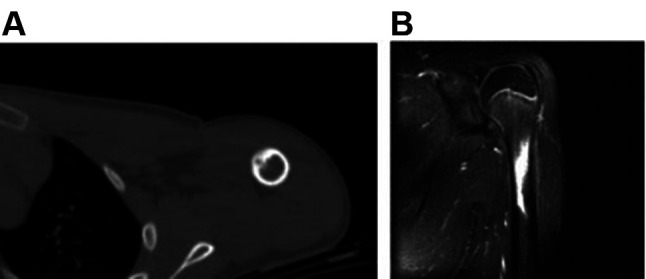
Osteoid osteoma, the third most common benign bone tumor, usually occurs in the cortex of long bones. It consists of a radiolucent nidus surrounded by reactive osteosclerosis. Generally, osteoid osteoma affects young males. Nocturnal pain that eases with salicylates or nonsteroidal anti-inflammatory drugs (NSAID) is the typical clinical presentation. Sometimes, it remains undiagnosed for a long time. Plain radiography and computed tomography are usually sufficient for the diagnosis of osteoid osteoma. Initial treatment includes salicylates and NSAID because the tumor often regresses spontaneously over 2-6 years. Surgical treatment is indicated in case of unresponsive pain to medical therapy, no tolerance of prolonged NSAID therapy due to side effects, and no willingness to activity limitations. Nowadays, minimally invasive techniques have replaced open surgery and are considered the gold standard of surgical treatment. Although cryoablation seems superior in terms of the nerve damage and immunotherapy effect, radiofrequency ablation is the preferred technique.
Keywords: en-bloc resection; imaging; medical therapy; percutaneous ablation; review; Οsteoid osteoma.
Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
Conflict of interest statement
The Authors report no conflicts of interest in relation to this study.
Figures
References
-
- Bednar MS, Weiland AJ, Light TR. Osteoid osteoma of the upper extremity. Hand Clin. 1995;11(2):211–221. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials