

Can you hear us now? The impact of health-care utilization by rare disease patients in the United States
- PMID: 34183788
- PMCID: PMC8553605
- DOI: 10.1038/s41436-021-01241-7
Can you hear us now? The impact of health-care utilization by rare disease patients in the United States
Abstract
Purpose: The vast majority of rare diseases (RDs) are complex, disabling, and life-threatening conditions with a genetic origin. RD patients face significant health challenges and limited treatments, yet the extent of their impact within health care is not well known. One direct method to gauge the disease burden of RDs is their overall cost and utilization within health-care systems.
Methods: The 2016 Healthcare Cost and Utilization Project (HCUP) databases were used to extract health-care utilization data using International Classification of Diseases, Tenth Revision (ICD-10) codes.
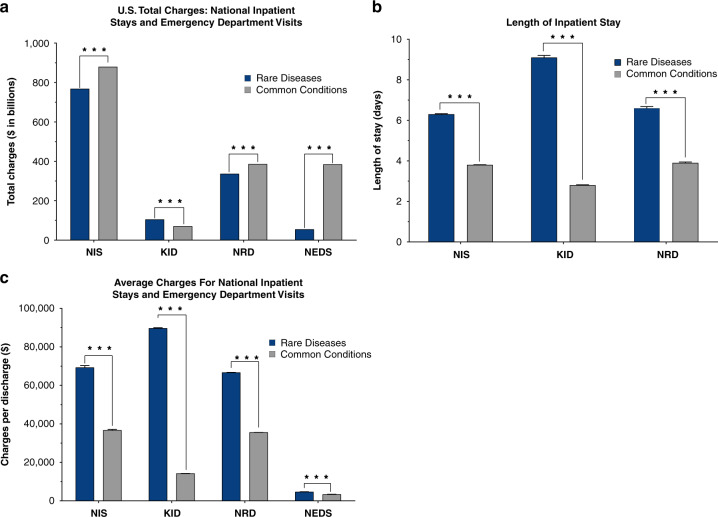
Results: Of 35.6 million national hospital weighted discharges in the HCUP Nationwide Inpatient Sample, 32% corresponded to RD-associated ICD-10 codes. Total charges were nearly equal between RDs ($768 billion) compared to common conditions (CCs) ($880 billion) (p < 0.0001). These charges were a result of higher charges per discharge and longer length of stay (LOS) for RD patients compared to those with CCs (p < 0.0001). Health-care cost and utilization was similarly higher for RDs with pediatric inpatient stays, readmissions, and emergency visits.
Conclusion: Pediatric and adult discharges with RDs show substantially higher health-care utilization compared to discharges with CCs diagnoses, accounting for nearly half of the US national bill.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Shah RR. Regulatory framework for the treatment of orphan diseases. In: Mehta A, Beck M, Sunder-Plassmann G, editors. Fabry Disease: Perspectives from 5 Years of FOS. Oxford. 2006.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
