

Peripartum cardiomyopathy in Iraq: initial registry-based data and 6 month outcomes
- PMID: 34184413
- PMCID: PMC8497348
- DOI: 10.1002/ehf2.13502
Peripartum cardiomyopathy in Iraq: initial registry-based data and 6 month outcomes
Abstract
Aims: This study aimed to evaluate the clinical characteristics, echocardiographic measurements, medical treatment, pregnancy outcomes, and the 6 month follow-up outcomes among patients with peripartum cardiomyopathy (PPCM) in Iraq.
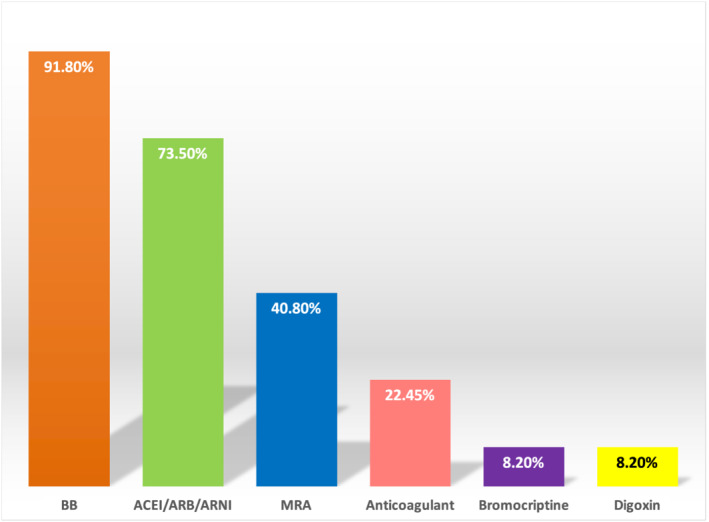
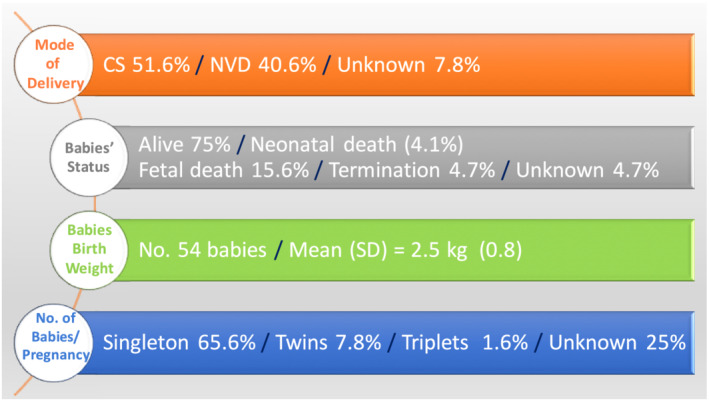
Methods and results: Data were collected prospectively at cardio-maternal clinic in Baghdad Heart Center, using case report form for the EORP-PPCM registry from January 2015 to November 2020. Six month follow-up was performed either by attendance of patients or by phone contact. A total of 64 PPCM patients were enrolled with a mean age of 32.1 ± 6.8 years. Diagnosis in 35 (54.7%) women was made in the post-partum period. There was a history of previous PPCM in 9 (14%), coexisting hypertension with the current pregnancy in 30 (51.7%), cholelithiasis in 5 (7.8%), and cancer in 3 (4.7%). Baseline mean left ventricular ejection fraction (LVEF) was 34.7 ± 8.1%, significantly higher than that reported globally (31 ± 10%) (P-value 0.011), and 26 (40.6%) of our patients had LVEF of ≤34%. Baseline mean global longitudinal strain (GLS) for 26 (40.6%) patients was -9.4 ± 4.1%. Baseline mean left ventricular end-diastolic and end-systolic dimensions were 61.2 ± 8.5 and 50.6 ± 10.2 mm, respectively. At 6 month follow-up, 11 (36.7%) women recovered their LVEF, lower than global data (46%) but higher than that in the Middle East (25%) with P-value 0.241 and 0.919, respectively. The mean LVEF was 44.5 ± 11.9%, and the mean GLS for 15 (23.4%) of patients was -13.4 ± 5.3%, including 5 (33.3%) with the range of -18.6% to -17%. Bromocriptine was the least used drug in 4 (8.2%) vs. globally reported (15%) (P-value 0.188). Thrombo-embolic events and maternal death were reported in 2 (4.1%) and 3 (4.7%) cases, respectively, within 6 months.
Conclusions: Around half of our PPCM patients were diagnosed at post-partum period with impaired initial LVEF and GLS, and one-third had early LVEF recovery at 6 month follow-up, higher than that in the Middle East but lower than the globally reported figure in the EORP-PPCM registry. Limited use of bromocriptine might explain the later finding. The co-morbid diseases in our setting were hypertension and cholelithiasis. Interestingly, the comparable ratios of neonatal and maternal mortalities in our study to that of the EORP-PPCM registry were found less than the Middle East figures. Bromocriptine needs to be considered in Middle East countries, including Iraq, which may be the key to improving LVEF recovery and perhaps reducing maternal mortality.
Keywords: Iraq; Mortality; Peripartum cardiomyopathy; Pregnancy.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Clinical presentation, management, and 6-month outcomes in women with peripartum cardiomyopathy: an ESC EORP registry.Eur Heart J. 2020 Oct 14;41(39):3787-3797. doi: 10.1093/eurheartj/ehaa455. Eur Heart J. 2020. PMID: 32840318 Free PMC article.
-
Pregnancies in women after peri-partum cardiomyopathy: the global European Society of Cardiology EuroObservational Research Programme Peri-Partum Cardiomyopathy Registry.Eur Heart J. 2025 Mar 13;46(11):1031-1040. doi: 10.1093/eurheartj/ehaf006. Eur Heart J. 2025. PMID: 39936475
-
Hypertensive disorders in women with peripartum cardiomyopathy: insights from the ESC EORP PPCM Registry.Eur J Heart Fail. 2021 Dec;23(12):2058-2069. doi: 10.1002/ejhf.2264. Epub 2021 Aug 25. Eur J Heart Fail. 2021. PMID: 34114268 Free PMC article.
-
Prognostic value of various markers in recovery from peripartum cardiomyopathy: a systematic review and meta-analysis.ESC Heart Fail. 2022 Oct;9(5):3483-3495. doi: 10.1002/ehf2.14085. Epub 2022 Jul 26. ESC Heart Fail. 2022. PMID: 35883253 Free PMC article.
-
Heart failure in pregnancy: what is the long-term impact of pregnancy on cardiac function? A tertiary care centre experience and systematic review.Open Heart. 2021 Aug;8(2):e001587. doi: 10.1136/openhrt-2021-001587. Open Heart. 2021. PMID: 34344721 Free PMC article.
Cited by
-
Thromboembolism in peripartum cardiomyopathy: a systematic review.J Thorac Dis. 2024 Jan 30;16(1):645-660. doi: 10.21037/jtd-23-945. Epub 2024 Jan 16. J Thorac Dis. 2024. PMID: 38410599 Free PMC article. Review.
-
The year in cardiovascular medicine 2021: heart failure and cardiomyopathies.Eur Heart J. 2022 Feb 3;43(5):367-376. doi: 10.1093/eurheartj/ehab887. Eur Heart J. 2022. PMID: 34974611 Free PMC article.
-
Hypertensive Disorders of Pregnancy and Peripartum Cardiomyopathy: A Meta-Analysis of Prevalence and Impact on Left Ventricular Function and Mortality.J Clin Med. 2025 Mar 4;14(5):1721. doi: 10.3390/jcm14051721. J Clin Med. 2025. PMID: 40095796 Free PMC article. Review.
References
-
- Farhan HA, Yaseen IF. Setting up a clinical service for PPCM in Iraq. In Sliwa K., ed. Peripartum Cardiomyopathy: From Pathophysiology to Management; 2021. p 93–114.
-
- Sliwa K, Mebazaa A, Hilfiker‐Kleiner D, Petrie MC, Maggioni AP, Laroche C, Regitz‐Zagrosek V, Schaufelberger M, Tavazzi L, van der Meer P, Roos‐Hesselink JW, Seferovic P, van Spandonck‐Zwarts K, Mbakwem A, Böhm M, Mouquet F, Pieske B, Hall R, Ponikowski P, Bauersachs J. Clinical characteristics of patients from the worldwide registry on peripartum cardiomyopathy (PPCM): EURObservational Research Programme in conjunction with the Heart Failure Association of the European Society of Cardiology Study Group on PPCM. Eur J Heart Fail 2017; 19: 1131–1141. - PubMed
-
- Sliwa K, Petrie MC, van der Meer P, Mebazaa A, Hilfiker‐Kleiner D, Jackson AM, Maggioni AP, Laroche C, Regitz‐Zagrosek V, Schaufelberger M, Tavazzi L, Roos‐Hesselink JW, Seferovic P, van Spaendonck‐Zwarts K, Mbakwem A, Böhm M, Mouquet F, Pieske B, Johnson MR, Hamdan R, Ponikowski P, Van Veldhuisen DJ, McMurray JJV, Bauersachs J. Clinical presentation, management, and 6‐month outcomes in women with peripartum cardiomyopathy: an ESC EORP registry. Eur Heart J 2020; 41: 3787–3797. - PMC - PubMed
-
- Hilfiker‐Kleiner D, Haghikia A, Masuko D, Nonhoff J, Held D, Libhaber E, Petrie MC, Walker NL, Podewski E, Berliner D, Bauersachs J, Sliwa K. Outcome of subsequent pregnancies in patients with a history of peripartum cardiomyopathy. Eur J Heart Fail 2017; 19: 1723–1728. - PubMed
-
- Bindi M, Bianchi M, Pinelli M, Castiglioni M. Scompenso cardiaco e calcolosi biliare [Heart failure and cholelithiasis]. Recenti Prog Med 2006; 97: 145 Italian. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
