

Analysis of Characteristics and Mortality in Cardiac Arrest Patients by Hospital Level: a Nationwide Population-based Study
- PMID: 34184437
- PMCID: PMC8239426
- DOI: 10.3346/jkms.2021.36.e173
Analysis of Characteristics and Mortality in Cardiac Arrest Patients by Hospital Level: a Nationwide Population-based Study
Abstract
Background: Survival and post-cardiac arrest care vary considerably by hospital, region, and country. In the current study, we aimed to analyze mortality in patients who underwent cardiac arrest by hospital level, and to reveal differences in patient characteristics and hospital factors, including post-cardiac arrest care, hospital costs, and adherence to changes in resuscitation guidelines.
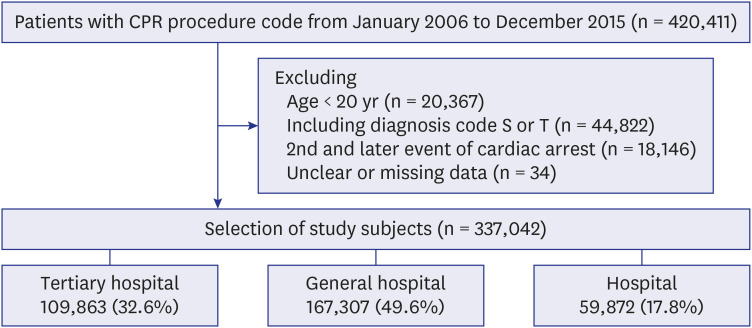
Methods: We enrolled adult patients (≥ 20 years) who suffered non-traumatic cardiac arrest from 2006 to 2015. Patient demographics, insurance type, admission route, comorbidities, treatments, and hospital costs were extracted from the National Health Insurance Service database. We categorized patients into tertiary hospital, general hospital, and hospital groups according to the level of the hospital where they were treated. We analyzed the patients' characteristics, hospital factors, and mortalities among the three groups. We also analyzed post-cardiac arrest care before and after the 2010 guideline changes. The primary end-point was 30 days and 1 year mortality rates.
Results: The tertiary hospital, general hospital, and hospital groups represented 32.6%, 49.6%, and 17.8% of 337,042 patients, respectively. The tertiary and general hospital groups were younger, had a lower proportion of medical aid coverage, and fewer comorbidities, compared to the hospital group. Post-cardiac arrest care, such as percutaneous coronary intervention, targeted temperature management, and extracorporeal membrane oxygenation, were provided more frequently in the tertiary and general hospital groups. After adjusting for age, sex, insurance type, urbanization level, admission route, comorbidities, defibrillation, resuscitation medications, angiography, and guideline changes, the tertiary and general hospital groups showed lower 1-year mortality (tertiary hospital vs. general hospital vs. hospital, adjusted odds ratios, 0.538 vs. 0.604 vs. 1; P < 0.001). After 2010 guideline changes, a marked decline in atropine use and an increase in post-cardiac arrest care were observed in the tertiary and general hospital groups.
Conclusion: The tertiary and general hospital groups showed lower 30 days and 1 year mortality rates than the hospital group, after adjusting for patient characteristics and hospital factors. Higher-level hospitals provided more post-cardiac arrest care, which led to high hospital costs, and showed good adherence to the guideline change after 2010.
Keywords: Cardiac Arrest; Cardiopulmonary Resuscitation; Guideline; Hospital Cost; Hospital Level; Mortality.
© 2021 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Wong CX, Brown A, Lau DH, Chugh SS, Albert CM, Kalman JM, et al. Epidemiology of sudden cardiac death: global and regional perspectives. Heart Lung Circ. 2019;28(1):6–14. - PubMed
-
- Gräsner JT, Herlitz J, Tjelmeland IB, Wnent J, Masterson S, Lilja G, et al. European Resuscitation Council Guidelines 2021: epidemiology of cardiac arrest in Europe. Resuscitation. 2021;161:61–79. - PubMed
-
- Korea Disease Control and Prevention Agency. Incidences of sudden cardiac arrest in Korea, 2019. [Updated 2021]. [Accessed April 10, 2021]. https://www.kdca.go.kr/upload_comm/syview/doc.html?fn=161295534263500.pd...
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
