

Ethnic differences in guideline-indicated statin initiation for people with type 2 diabetes in UK primary care, 2006-2019: A cohort study
- PMID: 34185782
- PMCID: PMC8241069
- DOI: 10.1371/journal.pmed.1003672
Ethnic differences in guideline-indicated statin initiation for people with type 2 diabetes in UK primary care, 2006-2019: A cohort study
Abstract
Background: Type 2 diabetes is 2-3 times more prevalent in people of South Asian and African/African Caribbean ethnicity than people of European ethnicity living in the UK. The former 2 groups also experience excess atherosclerotic cardiovascular disease (ASCVD) complications of diabetes. We aimed to study ethnic differences in statin initiation, a cornerstone of ASCVD primary prevention, for people with type 2 diabetes.
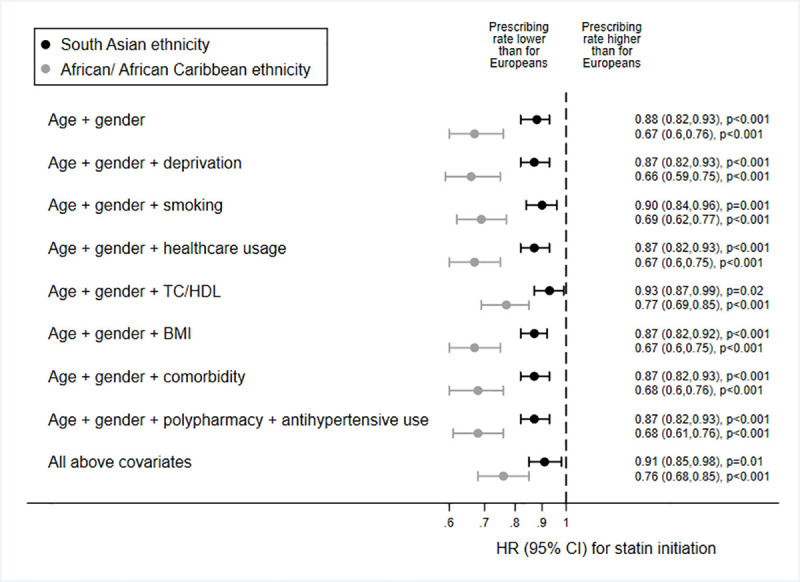
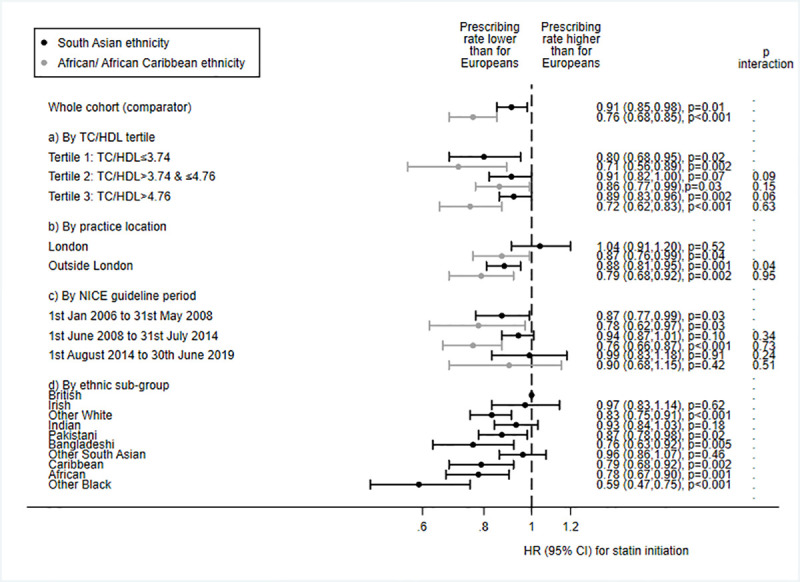
Methods and findings: Observational cohort study of UK primary care records, from 1 January 2006 to 30 June 2019. Data were studied from 27,511 (88%) people of European ethnicity, 2,386 (8%) people of South Asian ethnicity, and 1,142 (4%) people of African/African Caribbean ethnicity with incident type 2 diabetes, no previous ASCVD, and statin use indicated by guidelines. Statin initiation rates were contrasted by ethnicity, and the number of ASCVD events that could be prevented by equalising prescribing rates across ethnic groups was estimated. Median time to statin initiation was 79, 109, and 84 days for people of European, South Asian, and African/African Caribbean ethnicity, respectively. People of African/African Caribbean ethnicity were a third less likely to receive guideline-indicated statins than European people (n/N [%]: 605/1,142 [53%] and 18,803/27,511 [68%], respectively; age- and gender-adjusted HR 0.67 [95% CI 0.60 to 0.76], p < 0.001). The HR attenuated marginally in a model adjusting for total cholesterol/high-density lipoprotein cholesterol ratio (0.77 [95% CI 0.69 to 0.85], p < 0.001), with no further diminution when deprivation, ASCVD risk factors, comorbidity, polypharmacy, and healthcare usage were accounted for (fully adjusted HR 0.76 [95% CI 0.68, 0.85], p < 0.001). People of South Asian ethnicity were 10% less likely to receive a statin than European people (1,489/2,386 [62%] and 18,803/27,511 [68%], respectively; fully adjusted HR 0.91 [95% CI 0.85 to 0.98], p = 0.008, adjusting for all covariates). We estimated that up to 12,600 ASCVD events could be prevented over the lifetimes of people currently affected by type 2 diabetes in the UK by equalising statin prescribing across ethnic groups. Limitations included incompleteness of recording of routinely collected data.
Conclusions: In this study we observed that people of African/African Caribbean ethnicity with type 2 diabetes were substantially less likely, and people of South Asian ethnicity marginally less likely, to receive guideline-indicated statins than people of European ethnicity, even after accounting for sociodemographics, healthcare usage, ASCVD risk factors, and comorbidity. Underuse of statins in people of African/African Caribbean or South Asian ethnicity with type 2 diabetes is a missed opportunity to prevent cardiovascular events.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: RM reports a grant from the Wellcome Trust during the conduct of the study and personal fees from Amgen, outside the submitted work. NS has received grants and personal fees from Boehringer Ingelheim, and personal fees from Amgen, AstraZeneca, Eli Lilly, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer, and Sanofi outside the submitted work. LS has received grants from the British Heart Foundation and Diabetes UK during the conduct of the study, grants from the Wellcome Trust, Medical Research Council, National Institute for Health Research, GlaxoSmithKline, British Heart Foundation, Diabetes UK, the Newton Fund and UKRI, outside the submitted work, and is a non-executive director of the MHRA. KB has received grants from the Wellcome Trust and the Royal Society during the conduct of this study. NC has received grants from Diabetes UK during the conduct of this study and personal fees from AstraZeneca outside of the submitted work. SVE has no competing interests to declare.
Figures
References
-
- World Health Organization. Cardiovascular diseases: overview. Geneva: World Health Organization; 2020. [cited 2020 Nov 17]. Available from: https://www.who.int/health-topics/cardiovascular-diseases/#tab=tab_1.
-
- Tillin T, Hughes AD, Godsland IF, Whincup P, Forouhi NG, Welsh P, et al. Insulin resistance and truncal obesity as important determinants of the greater incidence of diabetes in Indian Asians and African Caribbeans compared with Europeans: the Southall And Brent REvisited (SABRE) cohort. Diabetes Care. 2013;36(2):383–93. doi: 10.2337/dc12-0544 - DOI - PMC - PubMed
-
- Tillin T, Hughes AD, Mayet J, Whincup P, Sattar N, Forouhi NG, et al. The relationship between metabolic risk factors and incident cardiovascular disease in Europeans, South Asians, and African Caribbeans: SABRE (Southall and Brent Revisited)—a prospective population-based study. J Am Coll Cardiol. 2013;61(17):1777–86. doi: 10.1016/j.jacc.2012.12.046 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
