

Rapidly Increasing Severe Acute Respiratory Syndrome Coronavirus 2 Seroprevalence and Limited Clinical Disease in 3 Malian Communities: A Prospective Cohort Study
- PMID: 34185847
- PMCID: PMC8394825
- DOI: 10.1093/cid/ciab589
Rapidly Increasing Severe Acute Respiratory Syndrome Coronavirus 2 Seroprevalence and Limited Clinical Disease in 3 Malian Communities: A Prospective Cohort Study
Abstract
Background: The extent of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) exposure and transmission in Mali and the surrounding region is not well understood. We aimed to estimate the cumulative incidence of SARS-CoV-2 in 3 communities and understand factors associated with infection.
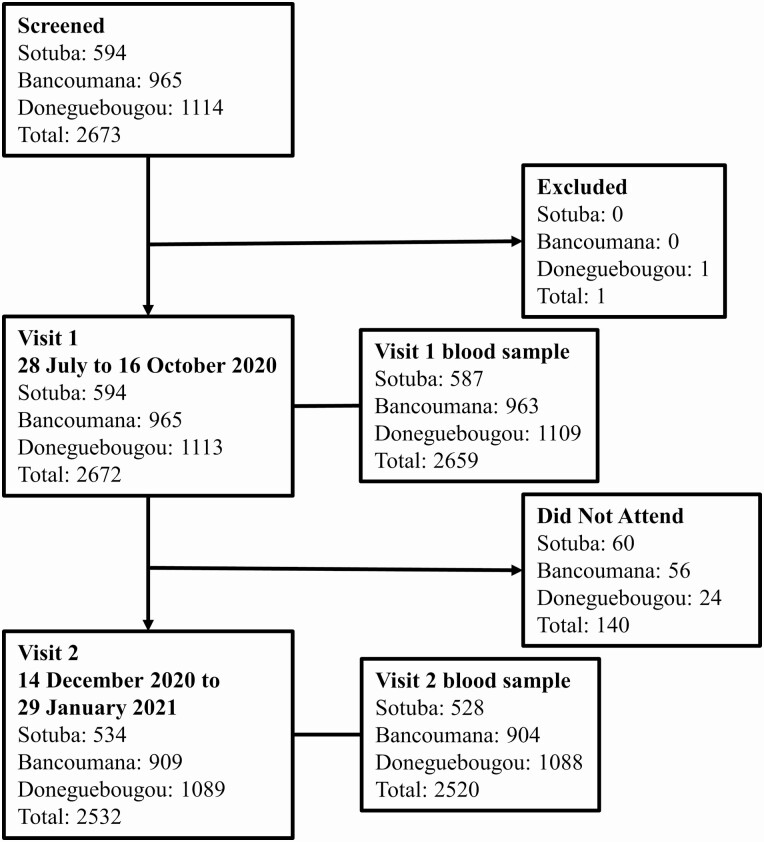
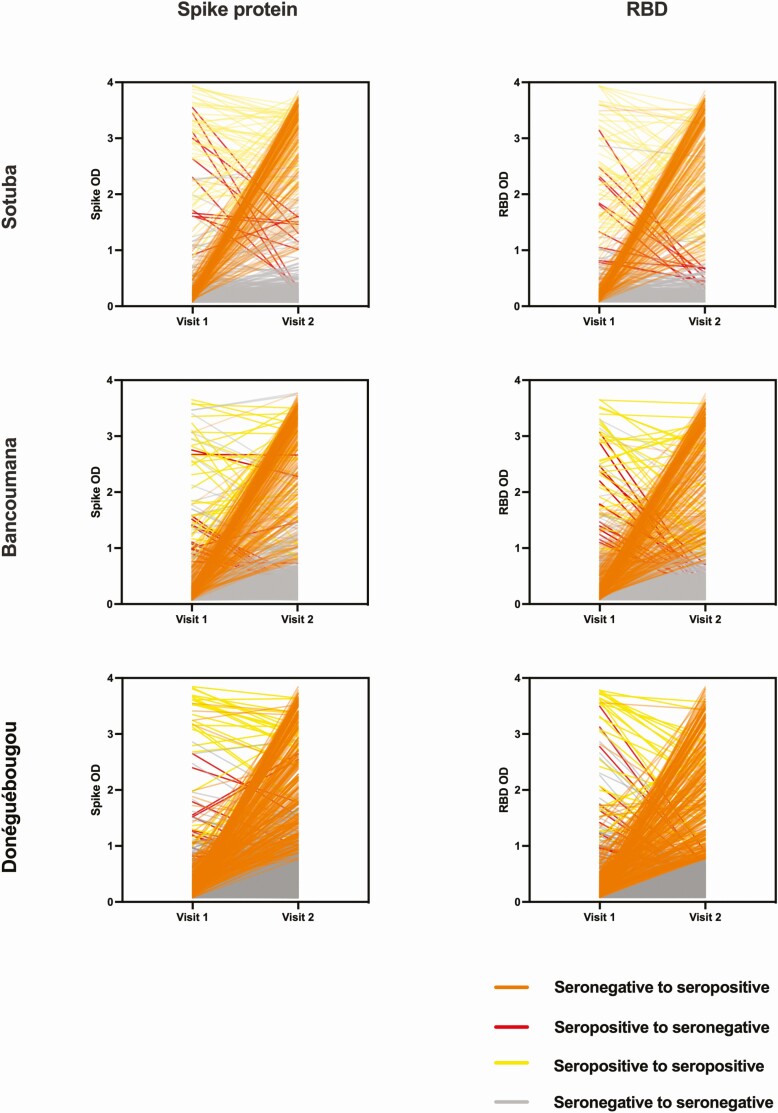
Methods: Between July 2020 and January 2021, we collected blood samples and demographic, social, medical, and self-reported symptoms information from residents aged 6 months and older over 2 study visits. SARS-CoV-2 antibodies were measured using a highly specific 2-antigen enzyme-linked immunosorbent assay optimized for use in Mali. We calculated cumulative adjusted seroprevalence for each community and evaluated factors associated with serostatus at each visit by univariate and multivariate analysis.
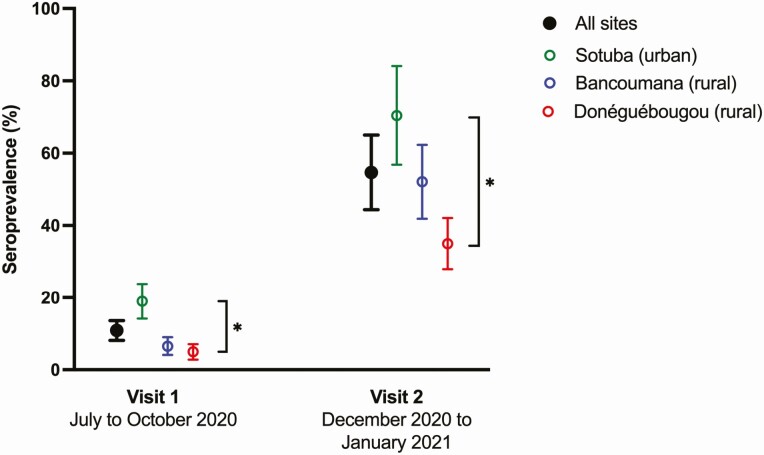
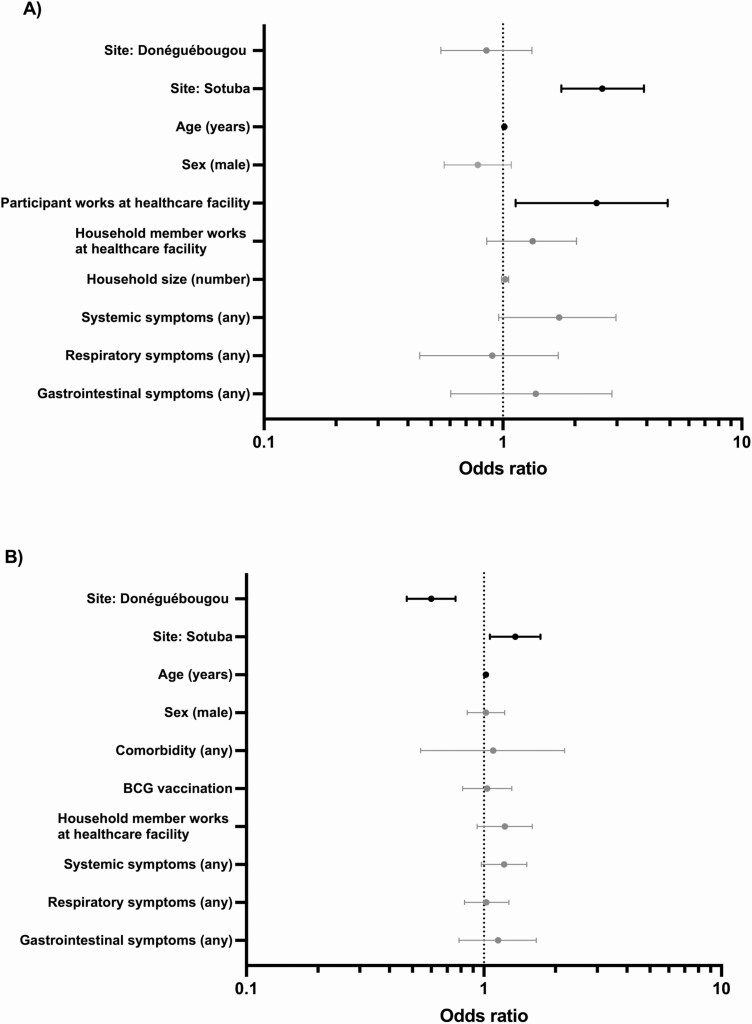
Results: Overall, 94.8% (2533/2672) of participants completed both study visits. A total of 31.3% (837/2672) were aged <10 years, 27.6% (737/2672) were aged 10-17 years, and 41.1% (1098/2572) were aged ≥18 years. The cumulative SARS-CoV-2 exposure rate was 58.5% (95% confidence interval, 47.5-69.4). This varied between sites and was 73.4% in the urban community of Sotuba, 53.2% in the rural town of Bancoumana, and 37.1% in the rural village of Donéguébougou. Study site and increased age were associated with serostatus at both study visits. There was minimal difference in reported symptoms based on serostatus.
Conclusions: The true extent of SARS-CoV-2 exposure in Mali is greater than previously reported and may now approach hypothetical "herd immunity" in urban areas. The epidemiology of the pandemic in the region may be primarily subclinical and within background illness rates.
Keywords: COVID-19; Mali; SARS-CoV-2; West Africa; seroprevalence.
Published by Oxford University Press for the Infectious Diseases Society of America 2021.
Figures
Update of
-
Rapidly increasing SARS-CoV-2 seroprevalence and limited clinical disease in three Malian communities: a prospective cohort study.medRxiv [Preprint]. 2021 Apr 29:2021.04.26.21256016. doi: 10.1101/2021.04.26.21256016. medRxiv. 2021. Update in: Clin Infect Dis. 2022 Mar 23;74(6):1030-1038. doi: 10.1093/cid/ciab589. PMID: 33948607 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
