

Oral administration of maternal vaginal microbes at birth to restore gut microbiome development in infants born by caesarean section: A pilot randomised placebo-controlled trial
- PMID: 34186487
- PMCID: PMC8254083
- DOI: 10.1016/j.ebiom.2021.103443
Oral administration of maternal vaginal microbes at birth to restore gut microbiome development in infants born by caesarean section: A pilot randomised placebo-controlled trial
Abstract
Background: Birth by caesarean section (CS) is associated with aberrant gut microbiome development and greater disease susceptibility later in life. We investigated whether oral administration of maternal vaginal microbiota to infants born by CS could restore their gut microbiome development in a pilot single-blinded, randomised placebo-controlled trial (Australian New Zealand Clinical Trials Registry, ACTRN12618000339257).
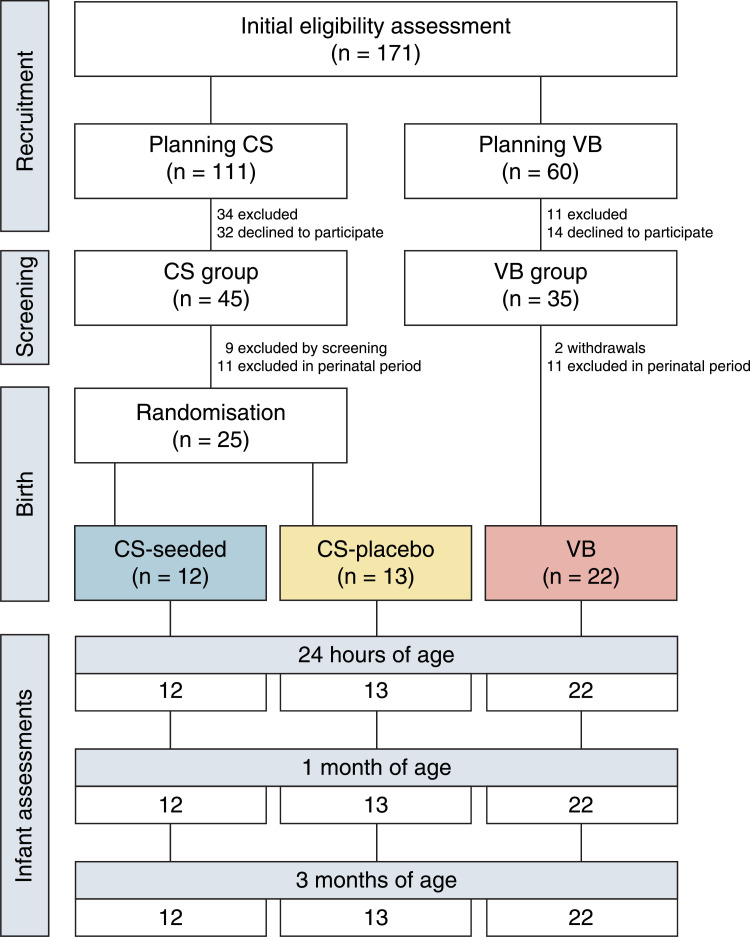
Methods: Pregnant women scheduled for a CS underwent comprehensive antenatal pathogen screening. At birth, healthy neonates were randomised to receive a 3 ml solution of either maternal vaginal microbes (CS-seeded, n = 12) or sterile water (CS-placebo, n = 13). Vaginally-born neonates were used as the reference control (VB, n = 22). Clinical assessments occurred within the first 2 h of birth, and at 1 month and 3 months of age. Infant stool samples and maternal vaginal extracts from CS women underwent shotgun metagenomic sequencing. The primary outcome was gut microbiome composition at 1 month of age. Secondary outcomes included maternal strain engraftment, functional potential of the gut microbiome, anthropometry, body composition, and adverse events.
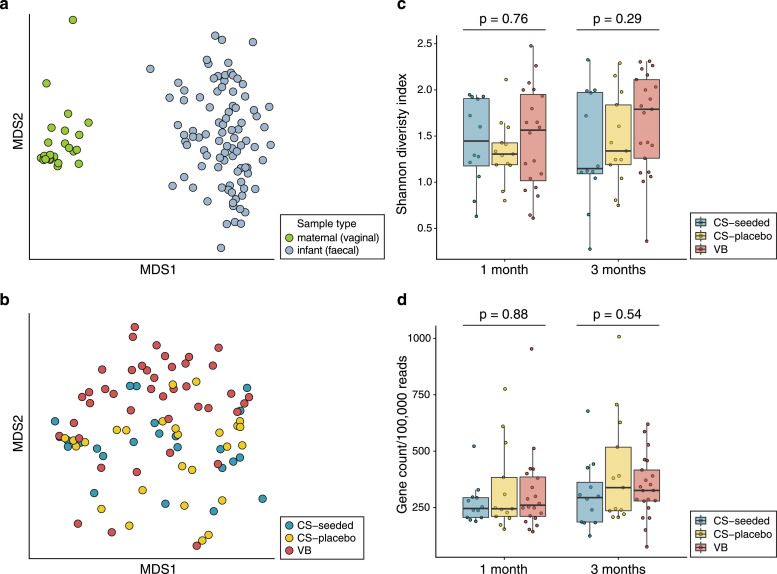
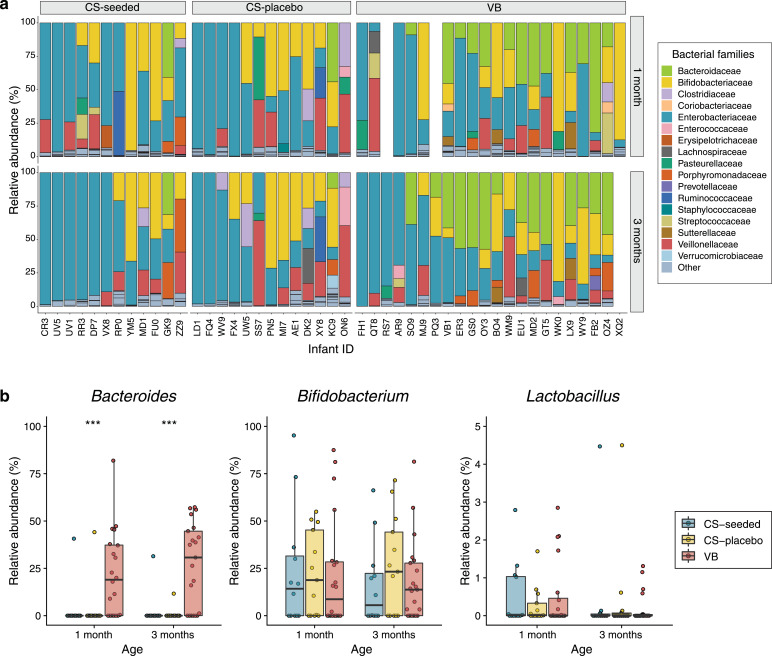
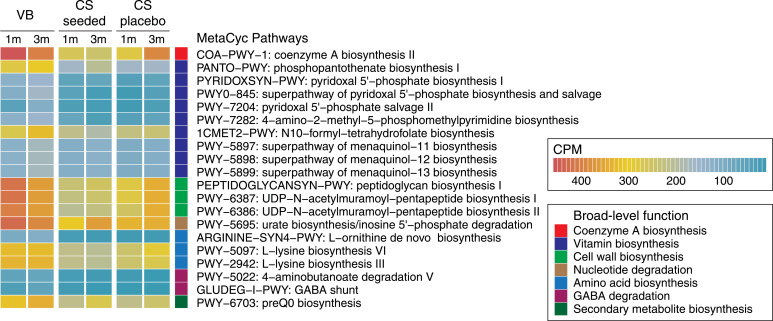
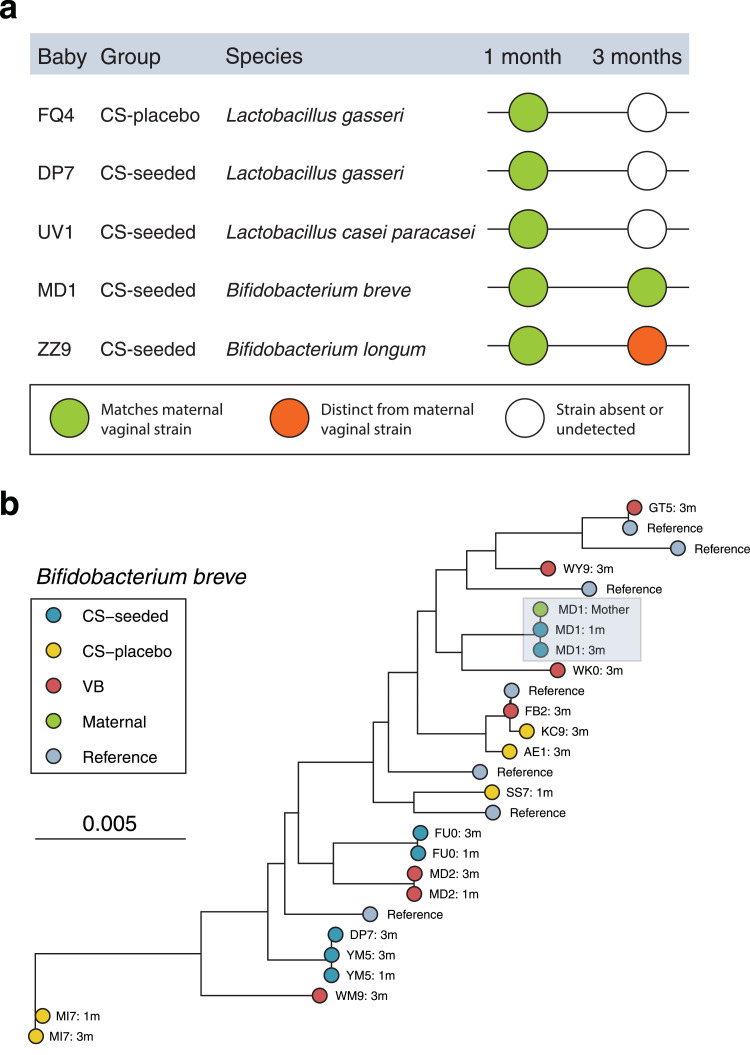
Findings: Despite the presence of viable microbial cells within transplant solutions, there were no observed differences in gut microbiome composition or functional potential between CS-seeded and CS-placebo infants at 1 month or 3 months of age. Both CS groups displayed the characteristic signature of low Bacteroides abundance, which contributed to a number of biosynthesis pathways being underrepresented when compared with VB microbiomes. Maternal vaginal strain engraftment was rare. Vaginal seeding had no observed effects on anthropometry or body composition. There were no serious adverse events associated with treatment.
Interpretation: Our pilot findings question the value of vaginal seeding given that oral administration of maternal vaginal microbiota did not alter early gut microbiome development in CS-born infants. The limited colonisation of maternal vaginal strains suggest that other maternal sources, such as the perianal area, may play a larger role in seeding the neonatal gut microbiome.
Funding: Health Research Council of New Zealand, A Better Start - National Science Challenge.
Keywords: Birth; Caesarean section; Gut microbiome; Infant development; Maternal strain transmission; Metagenomics; Vaginal seeding.
Copyright © 2021. Published by Elsevier B.V.
Conflict of interest statement
Declaration of Competing Interest The authors have nothing to disclose.
Figures
Similar articles
-
Maternal bacteria to correct abnormal gut microbiota in babies born by C-section.Medicine (Baltimore). 2020 Jul 24;99(30):e21315. doi: 10.1097/MD.0000000000021315. Medicine (Baltimore). 2020. PMID: 32791721 Free PMC article. Clinical Trial.
-
The influence of maternal gut and vaginal microbiota on gastrointestinal colonization of neonates born vaginally and per caesarean section.BMC Pregnancy Childbirth. 2025 Mar 8;25(1):254. doi: 10.1186/s12884-025-07358-w. BMC Pregnancy Childbirth. 2025. PMID: 40057706 Free PMC article.
-
Birth Mode Does Not Determine the Presence of Shared Bacterial Strains between the Maternal Vaginal Microbiome and the Infant Stool Microbiome.Microbiol Spectr. 2023 Aug 17;11(4):e0061423. doi: 10.1128/spectrum.00614-23. Epub 2023 Jun 20. Microbiol Spectr. 2023. PMID: 37338388 Free PMC article.
-
Impact of vaginal seeding on the gut microbiome of infants born via cesarean section: A systematic review.J Infect. 2024 Dec;89(6):106348. doi: 10.1016/j.jinf.2024.106348. Epub 2024 Nov 12. J Infect. 2024. PMID: 39537035
-
Gut Microbiota Composition in Healthy Japanese Infants and Young Adults Born by C-Section.Ann Nutr Metab. 2018;73 Suppl 3:4-11. doi: 10.1159/000490841. Epub 2018 Jul 24. Ann Nutr Metab. 2018. PMID: 30041174 Review.
Cited by
-
The Role of Early Life Microbiota Composition in the Development of Allergic Diseases.Microorganisms. 2022 Jun 9;10(6):1190. doi: 10.3390/microorganisms10061190. Microorganisms. 2022. PMID: 35744708 Free PMC article. Review.
-
From Short- to Long-Term Effects of C-Section Delivery on Microbiome Establishment and Host Health.Microorganisms. 2021 Oct 9;9(10):2122. doi: 10.3390/microorganisms9102122. Microorganisms. 2021. PMID: 34683443 Free PMC article. Review.
-
Microbiota transplantation in restoring cesarean-related infant dysbiosis: a new frontier.Gut Microbes. 2024 Jan-Dec;16(1):2351503. doi: 10.1080/19490976.2024.2351503. Epub 2024 May 15. Gut Microbes. 2024. PMID: 38748594 Free PMC article.
-
Environmental Interventions for Preventing Atopic Diseases.Curr Allergy Asthma Rep. 2024 May;24(5):233-251. doi: 10.1007/s11882-024-01141-1. Epub 2024 Mar 16. Curr Allergy Asthma Rep. 2024. PMID: 38492159 Review.
-
More than just a number: the gut microbiota and brain function across the extremes of life.Gut Microbes. 2024 Jan-Dec;16(1):2418988. doi: 10.1080/19490976.2024.2418988. Epub 2024 Nov 20. Gut Microbes. 2024. PMID: 39567371 Free PMC article. Review.
