

Class II correction by maxillary en masse distalization using a completely customized lingual appliance and a novel mini-screw anchorage concept - preliminary results
- PMID: 34187487
- PMCID: PMC8240392
- DOI: 10.1186/s13005-021-00273-3
Class II correction by maxillary en masse distalization using a completely customized lingual appliance and a novel mini-screw anchorage concept - preliminary results
Abstract
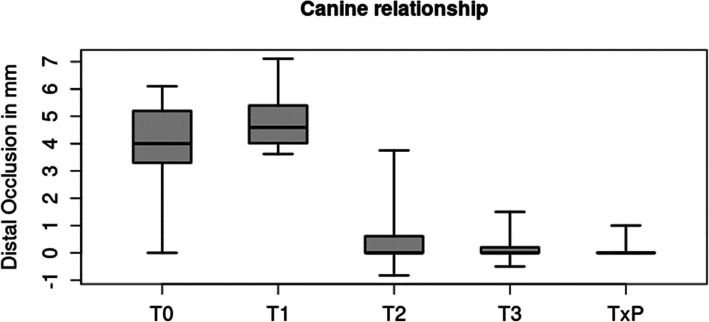
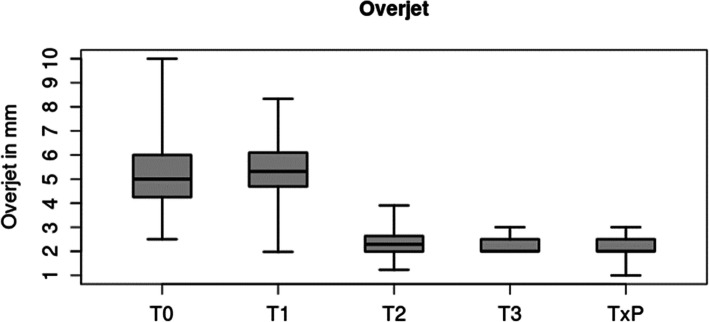
Background: The aim of the study was to evaluate the efficacy of a novel en masse distalization method in the maxillary arch in combination with a completely customized lingual appliance (CCLA; WIN, DW Lingual Systems, Germany). Therefore, we tested the null-hypothesis of a significant deviation from an Angle-Class I canine relationship and a normal overjet defined by an individual target set-up after dentoalveolar compensation in Angle Class II subjects.
Methods: This retrospective study included 23 patients, (m/f 3/20, mean age 29.6 years (min/max, 13.6/50.9 years)), with inclusion criteria of an Angle Class II occlusion of more than half a cusp prior to en masse distalization and treatment completed consecutively with a CCLA in combination with a mini-screw (MS) anchorage for uni- or bilateral maxillary distalization (12 bilateral situations, totalling 35). Plaster casts taken prior to (T0) and following CCLA treatment (T3) were compared with the treatment plan / set-up (TxP, with a Class I canine relationship and a normal overjet as the treatment objective). MSs were placed following levelling and aligning (T1) and removed at the end of en masse distalization at T2. Statistical analysis was carried out using Schuirmann's TOST [two one-sided tests] equivalence test, based on a one-sample t-test with α = 0.025 on each side (total α = 0.05).
Results: Ninety-seven percent of planned correction of the canine relationship was achieved (mean 3.6 of 3.7 mm) and also 97 % of the planned overjet correction (mean 3.1 of 3.2 mm), with a statistically significant equivalence (p < 0.0001) for canine relationship and overjet between the individual treatment plan (set-up) and the final outcome. Adverse effects were limited to the loss of n = 2 of 35 mini-screws. However, in each instance, the treatment was completed, as scheduled, without replacing them. Accordingly, the null-hypothesis was rejected.
Conclusions: The technique presented allows for a predictable correction of an Angle-Class II malocclusion via dentoalveolar compensation with maxillary en masse distalization.
Keywords: Anchorage; Class II correction; Distalization; Lingual appliances; Lingual orthodontics; Mini-screws; TADs.
Conflict of interest statement
DW is the inventor of the WIN system. The WIN system is manufactured by DW Lingual Systems and DW is the CEO of this company. All other authors declare that they have no competing interests.
Figures



References
-
- Angle EH. The Angle system of regulation and retention of the teeth, and treatment of fractures of the maxillae. 5th ed. Philadelphia: The S. S. White Dental mfg. co.; 1897;iii:5-111.
-
- Bae SM, Park HS, Kyung HM, Kwon OW, Sung JH. Clinical application of micro-implant anchorage. J Clin Orthod. 2002;36(5):298–302. - PubMed
-
- Kanomi R. Mini-implant for orthodontic anchorage. J Clin Orthod. 1997;31(11):763–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
