

Non-invasive plasma glycomic and metabolic biomarkers of post-treatment control of HIV
- PMID: 34188039
- PMCID: PMC8241829
- DOI: 10.1038/s41467-021-24077-w
Non-invasive plasma glycomic and metabolic biomarkers of post-treatment control of HIV
Abstract
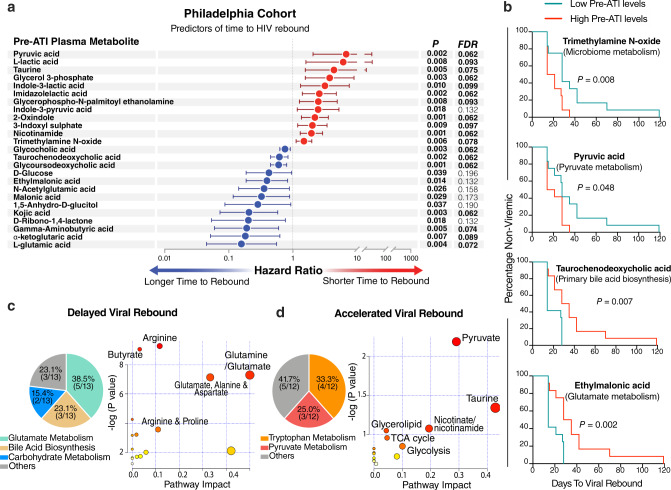
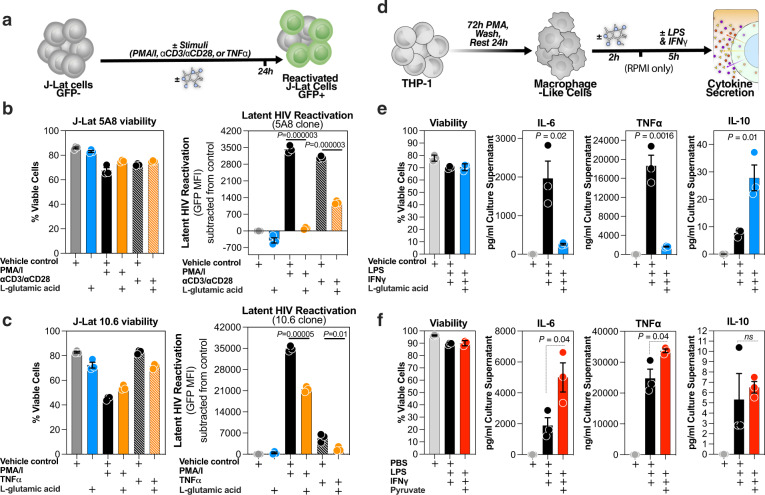
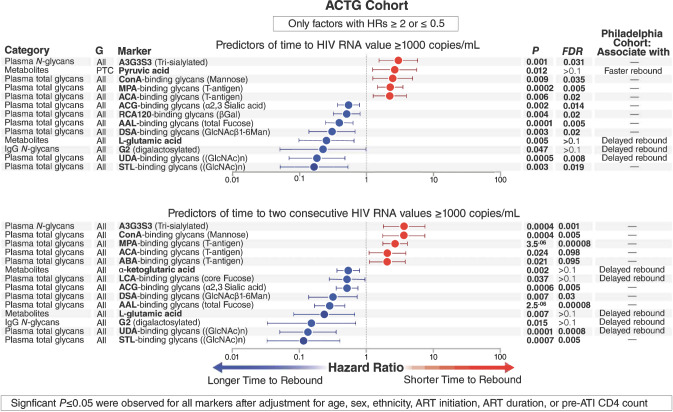
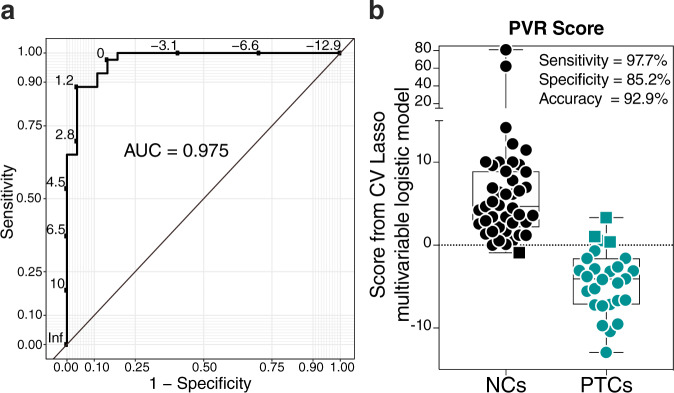
Non-invasive biomarkers that predict HIV remission after antiretroviral therapy (ART) interruption are urgently needed. Such biomarkers can improve the safety of analytic treatment interruption (ATI) and provide mechanistic insights into the host pathways involved in post-ART HIV control. Here we report plasma glycomic and metabolic signatures of time-to-viral-rebound and probability-of-viral-remission using samples from two independent cohorts. These samples include a large number of post-treatment controllers, a rare population demonstrating sustained virologic suppression after ART-cessation. These signatures remain significant after adjusting for key demographic and clinical confounders. We also report mechanistic links between some of these biomarkers and HIV latency reactivation and/or myeloid inflammation in vitro. Finally, machine learning algorithms, based on selected sets of these biomarkers, predict time-to-viral-rebound with 74% capacity and probability-of-viral-remission with 97.5% capacity. In summary, we report non-invasive plasma biomarkers, with potential functional significance, that predict both the duration and probability of HIV remission after treatment interruption.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
- UM1 AI126620/AI/NIAID NIH HHS/United States
- R21 NS106970/NS/NINDS NIH HHS/United States
- R01 AG062383/AG/NIA NIH HHS/United States
- R01 DK123733/DK/NIDDK NIH HHS/United States
- UM1 AI069534/AI/NIAID NIH HHS/United States
- R21 AI129636/AI/NIAID NIH HHS/United States
- R01 NS117458/NS/NINDS NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- R01 AI165079/AI/NIAID NIH HHS/United States
- S10 OD023586/OD/NIH HHS/United States
- R01 AI048398/AI/NIAID NIH HHS/United States
- R21 AI143385/AI/NIAID NIH HHS/United States
- P30 CA010815/CA/NCI NIH HHS/United States
- R50 CA221838/CA/NCI NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
